
![]()
Bartholin's Gland Cyst Marsupialization
Excision of Vulvar Skin, with Split-Thickness Skin Graft
Vaginal Outlet Stenosis Repair
Closure of Wide Local Excision of the Vulva
Wide Local Excision of the Vulva, With Primary Closure or Z-plasty Flap
Alcohol Injection of the Vulva
Cortisone Injection of the Vulva
Excision of the Vulva by the Loop Electrical Excision Procedure (LEEP)
Excision Of Hypertrophied Clitoris
Clitoral hypertrophy, regardless of etiology, is a source of psychological stress, especially in young females. Most pediatric gynecologists stress the importance of normal external genitalia in young children. It is important to weigh the role of the clitoris in sexual climax against the psychological stress incurred when the genitalia of a young child are different from her peers.
The purpose of the operation is to excise the hypertrophied clitoris and create normal-appearing external genitalia.
Pathophysiologic Changes: Patients should be counseled about potential neurological damage and loss of sensation. Although the clitoris is a major source of sexual stimulation, many patients who have had a complete vulvectomy achieve satisfactory sexual climax without the clitoris.
Points of Caution: Excision of the clitoris is simple, but bleeding from the plexus of veins at the base of the clitoris can be considerable, and meticulous care must be taken to ensure hemostasis.
Technique
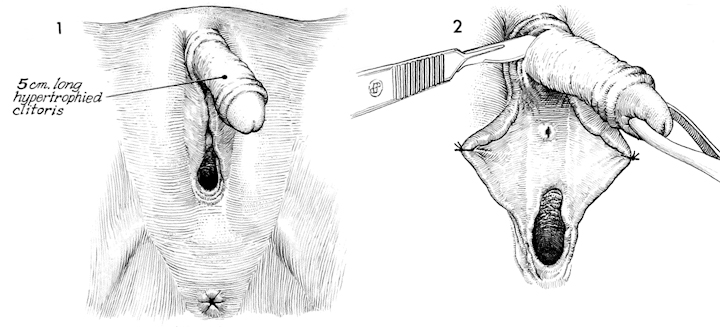
A 5 cm-hypertrophied clitoris is shown.
2. The end of the clitoris is grasped with an Allis clamp and placed on traction. A small scalpel is used to wedge resect the clitoris from the labial fold.
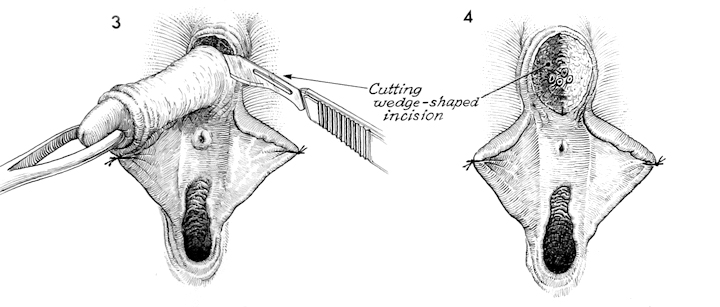
3. A wedge incision is completed on the opposite side.
4. A fish-mouth defect is created. The network of venous sinusoids located in the base of the clitoris requires that meticulous hemostasis be achieved to avoid large vulvar hematomas. Because clamping each venous sinusoid is difficult , suture ligation of the sinusoids can be performed by using 4/0 absorbable suture on a fine gastrointestinal needle and placing a stitch deep within the sinusoidal area. The suture can then be used as a retractor to lift the vascular tissue upward. Additional locking sutures can be placed in the base of the bleeding area until hemostasis has been achieved.
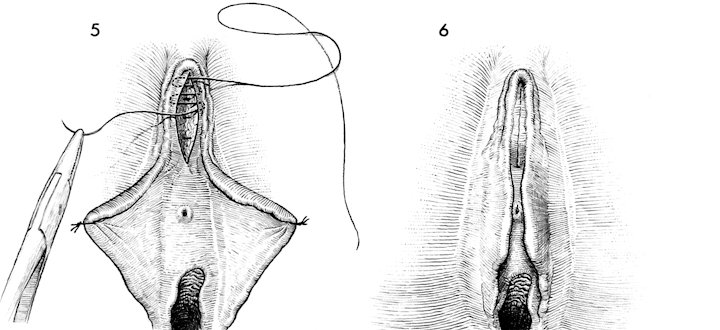
5. The defect is closed in layers of fine absorbable suture with the final layer being placed as subcuticular stitches.
6. When complete, the operation results in the normal appearance of the external genitalia.