
![]()
Diagnostic Uses of Laparoscopy
Demonstration of Tubal Patency via Laparoscopy
Laparoscopic Resection of Unruptured Ectopic Pregnancy
Ovarian Biopsy via Laparoscopy
Electrocoagulation of Endometriosis via Laparoscopy
Lysis or Adhesions via Laparoscopy
Control of Hemorrhage During Laparoscopy
Sterilization by Electrocoagulation and Division via Laparoscopy
Silastic Band Sterilization via Laparoscopy
Hulka Clip Sterilization via Laparoscopy
Sterilization by the Pomeroy Operation
Sterilization by the Modified Irving Technique
Sterilization by the Minilaparotomy Technique
Sterilization - Ucheda Technique
Tuboplasty - Microresection and Anastomosis of the Fallopian Tube
Sterilization - Ucheda Technique
The Ucheda operation is performed through a mini-laparotomy incision. Its advantage over mini-laparotomy, Pomeroy, and laparoscopy techniques has not been demonstrated, but theoretically the main advantage is that the distal portion of the fallopian tube is exteriorized through the peritoneum, while the proximal portion of the fallopian tube is buried within the broad ligament. On thin, small patients, it can be performed through a 4-cm incision similar to that of the mini-laparotomy technique.
The purpose is to obstruct the fallopian tubes and prevent pregnancy.
Pathophysiologic Changes: The proximal segment of the distal portion of the fallopian tube is exteriorized so that any oocyte entering the fimbriated end of the fallopian tube is rapidly expelled into the peritoneal cavity. This would also occur if the suture on the proximal portion of the distal segment became dislodged or if that segment reopens via a tubo-peritoneal fistula. The distal portion of the proximal segment of the fallopian tube is buried deep within the broad ligament.
Points of Caution: The saline solution must be injected carefully so that only the peritoneal covering of the fallopian tube is hydraulically elevated in a blister fashion. Care must be taken to identify the fallopian tube and ligate it completely.
Technique
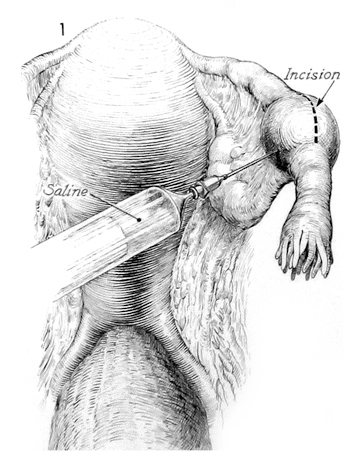
The abdomen has been opened through a transverse incision as in a mini-laparotomy technique. The fallopian tube is grasped with a Babcock clamp and elevated into the abdominal incision. The serosal covering of the tube is injected with saline solution. A longitudinal incision is made in the serosa over the area injected with the saline solution.
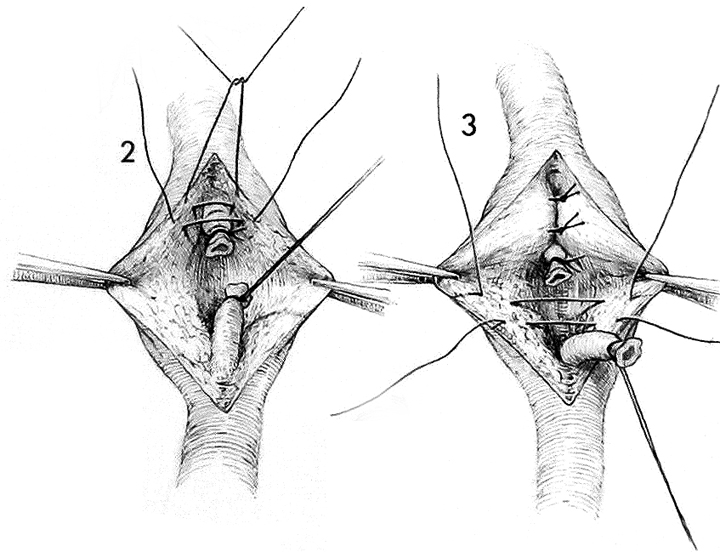
The fallopian tube is dissected out and a piece is removed between ties of 3/0 silk suture. The distal segment of the proximal portion of the fallopian tube is buried within the wound which is rapidly closed with interrupted 3/0 synthetic absorbable sutures.
The proximal segment of the distal portion of the fallopian tube is exteriorized through the serosal opening.
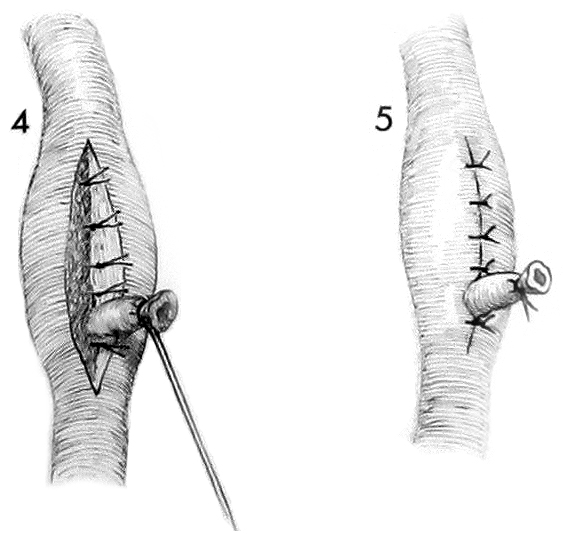
Closure of the wound is competed with exteriorization of the proximal segment of the distal portion of the tube.
The serosa is closed with several fine 3/0 synthetic absorbable sutures. The abdomen is then closed in layers.