
Abdominal
Wall
Pfannenstiel Incision
Maylard Incision
Panniculectomy
Incisional Hernia
Repair
Abdominal
Wound
Dehiscence and
Evisceration
Massive
Closure
of the Abdominal
Wall With a One-Knot
Loop Suture
Hemorrhage
Control Following Laceration
of Inferior Upper
Epigastric Vessels |
Panniculectomy
A large abdominal panniculus after weight reduction in a patient who
has had excessive obesity can be associated with excoriation and breakdown
of the underside of the panniculus. In these cases, panniculectomy
is indicated.
The purpose of panniculectomy is to remove the large abdominal
panniculus.
Physiologic Changes. Large
panniculi will frequently contain 500-700 mL of blood within the
mass of tissue. Therefore, this procedure can be associated with
excessive blood loss. Postoperative hypovolemia and its clinical
sequelae may result.
Points of Caution. The patient should
be evaluated in both the standing and the supine position prior to
the operation to design an incision that will prevent the "dog ears"
that frequently occur after a panniculectomy in the area of the anterior
iliac spine.
One assistant must be constantly available to keep traction on the
panniculus.
Meticulous attention to hemostasis is essential. The wound should be
drained with suction catheters.
Technique
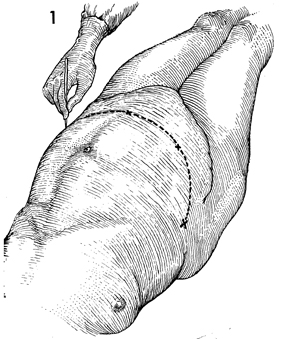
The patient is placed in the dorsal supine
position. Brilliant green surgical dye is used to design and
mark off the lines of incision. |
Large fishhooks are inserted
into the panniculus and connected to an orthopedic frame erected
over the operating table to elevate the panniculus. The inferior
margin of the panniculus can be marked. A V-shaped incision over
the mons pubis and Z-shaped incision at the lateral margins are
made to prevent overlapping of the abdominal flaps and the "dog
ear" protrusion of tissue at the iliac spines. |
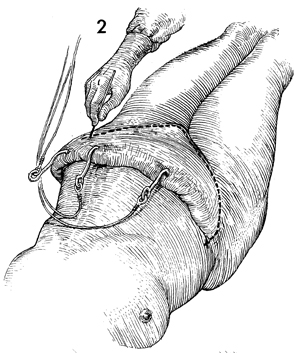
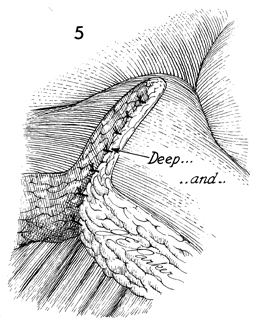
While the flap is held on traction with fishhooks,
the incisions are carried down to the rectus fascia. |
Unless meticulous hemostasis
is maintained throughout the operation, blood loss will become
excessive. The V-shaped incision in the mons pubis should be
closed with interrupted 2-0 synthetic absorbable sutures. |
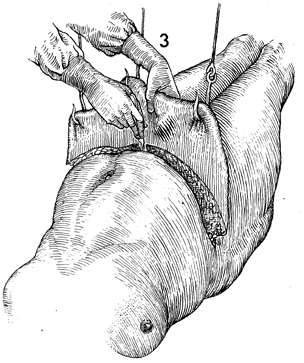
The reconstruction of the mons pubis has
been completed with placement of the subcutaneous row of interrupted
3-0 synthetic absorbable sutures. |
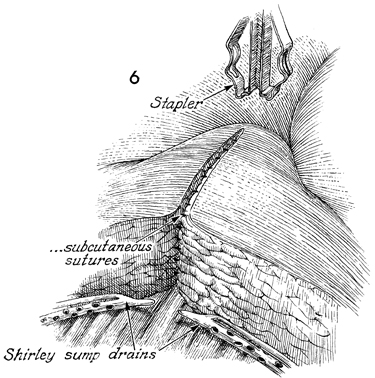
Suction drains are placed
in the wound and may be anchored to the rectus fascia with a
5-0 synthetic absorbable suture to prevent displacement. The
skin stapler is used to close the edge of the wound. |
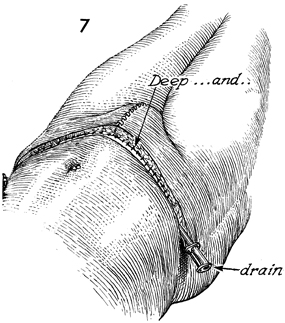
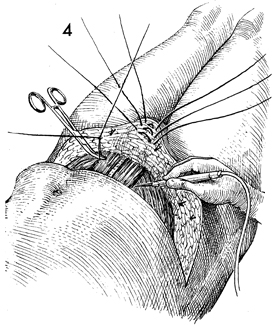
The cephalad margin of the abdominal flap
should be mobilized up to the umbilicus. If a great deal of mobilization
is required, an elliptical incision can be made around the umbilicus,
and a matching elliptical defect can be created cephalad to the
umbilicus. Then, when the abdominal wall is completely mobilized
and moved caudad to match the inferior margin of the incision,
the elliptical umbilical incision can be closed, and the umbilicus
can be sutured to the edges of the newly created abdominal defect.
The abdominal incision should be closed with interrupted 2-0
synthetic absorbable sutures. |
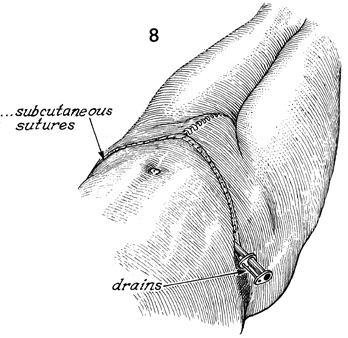
A second layer of subcutaneous sutures is
placed with 3-0 synthetic absorbable sutures. |
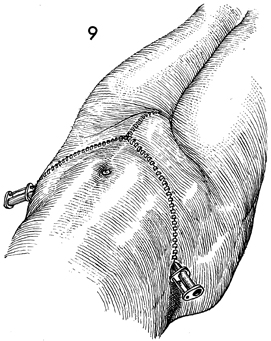
The remaining portions of the skin are approximated
with stainless steel skin clips. The suction drains are connected
to continuous suction. They are removed when they are no longer
productive. |
|
|
