|
||||||
Abdominal
Wound Massive
Closure Hemorrhage
Control Following Laceration |
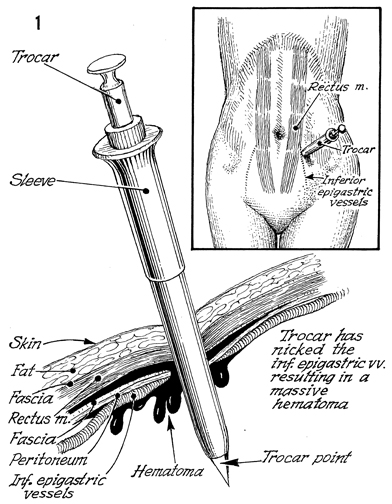
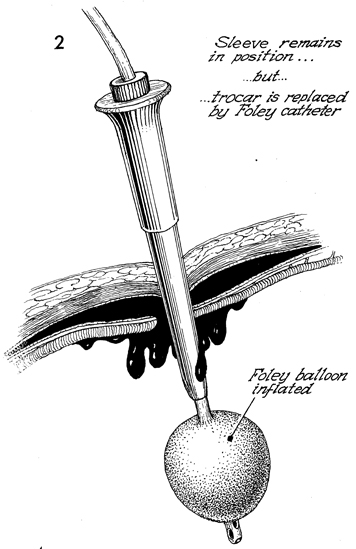
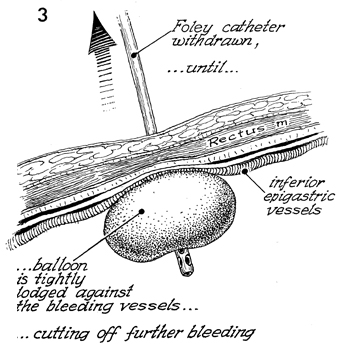
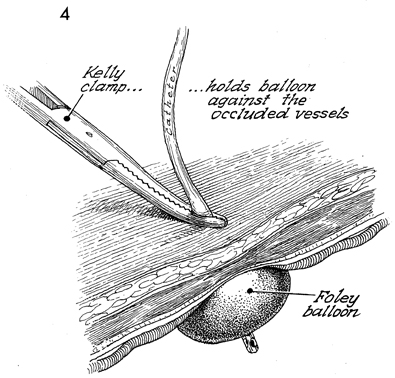
Hemorrhage Control Following With the use of multiple trocar insertion through the abdominal wall, especially the left and right lower quadrants of the abdomen, there is a significant chance of the trocar injuring the inferior epigastric vessels located on the lateral aspects of the rectus abdominis muscle. Laceration of these vessels creates a significant abdominal wall hematoma. If the tears in the subfascia and peritoneum are significant, uncontrolled bleeding from the inferior epigastric vessels may enter the peritoneal cavity, and the patient could progress into hypovolemic shock without the appearance of an abdominal wall hematoma. Before resorting to a laparotomy to control the bleeding, the surgeon is advised to first attempt hemorrhage control with a simple procedure using equipment available in any hospital, i.e., a Foley catheter and Kelly clamp. Physiologic Changes. The changes are those of blood loss. Points of Caution. Care must be utilized to select a Foley catheter that will easily fit the trocar sheath. After the hemorrhage has been controlled, the patient must be admitted to the hospital for close observation to ensure that the inferior epigastric vessels are adequately entrapped between the balloon of the Foley catheter and the Kelly clamp placed adjacent to the skin. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.