
Colon
Appendectomy
Appendectomy
Using
the Linear Dissecting
Stapler
Transverse
Loop
Colostomy
End
Sigmoid Colostomy With Hartmann's Pouch
Closure
of a Loop
Colostomy
Anterior
Resection
of the Colon With Low
Anastomosis Using
the Gambee Suture
Technique
Low
Anastomosis
of Colon to Rectum
Using the End-to-End
Surgical Stapler
Technique
Anterior
Resection
of the Colon With
Low Anastomosis via
the Strasbourg-Baker
Technique |
Closure of a Loop Colostomy
Closure of a loop colostomy is facilitated if the posterior
wall of the colon has been transected. If it has been transected, a
classical colocolostomy is required.
The purpose of this operation is
to close the colostomy and reestablish continuity of the colon without
stricture at the site of the anastomosis.
Physiologic Changes. After
this procedure, the patient may resume defecation per anum. In addition,
the patient will receive more nutritive value from food because the
additional colonic surface will allow greater absorption of water
and nutrients from the intestinal contents.
Points of Caution. Care must be taken
to prevent stenosis at the anastomotic site. If the diameter of the
anastomosis is less than 2 cm, the anastomosis should be taken down
and resected. A classic end-to-end anastomosis should be performed
to ensure adequate diameter to the intestine. If the posterior wall
of the colon has been preserved, care should be taken to close the
colostomy prior to opening the peritoneal cavity. This will reduce
intraperitoneal contamination from the stoma site.
Copious irrigation
of the wound should be made prior to primary closure. If gross contamination
has occurred, delayed closure of the wound should be considered.
Technique
The patient should have a thorough surgical
bowel prep prior to closure of the colostomy. This should consist
of a clear liquid diet, a nonabsorbable antibiotic (such as neomycin
and Sulfathalidine), and a thorough mechanical cleansing of the
bowel.
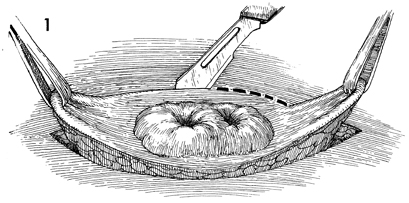
The patient is placed in the
supine position, and adequate anesthesia is administered. The
abdomen is surgically prepared, and an elliptical incision is
made in the skin approximately 2 cm from the margin of the colostomy
stoma. This incision is carried down to the rectus fascia, but
no farther. |
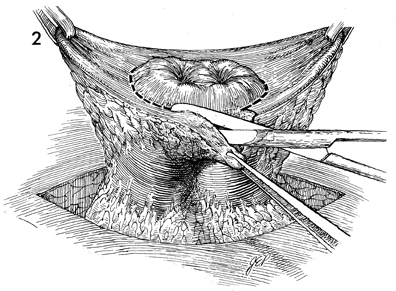
After the incision has been made, Allis clamps
are applied to the ends of the elliptical incision, and traction
is applied upward. A sharp Metzenbaum scissors is used to trim
excessive skin away from the margin of the bowel. Adhesions between
the serosal surface of the bowel and rectus fascia are lysed
by sharp dissection. |
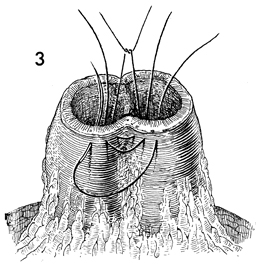
The bowel has been prepped for a Gambee single-layer
through-and-through anastomosis. Synthetic absorbable sutures
are placed through the wall of the bowel, starting on the mucosa,
exiting through the serosa, reentering the serosa on the opposite
side, and exiting through the mucosa of the opposite side. Thus
the knot will be tied in the lumen of the bowel. |
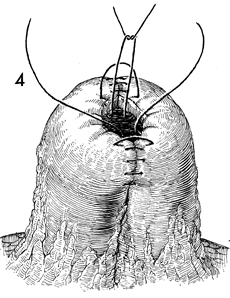
The Gambee anastomosis is near its
completion with an inverting suture technique.
|
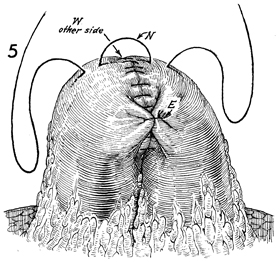
When the Gambee anastomosis has been completed,
several Lembert sutures are placed north (N), east (E), and west
(W) to relieve tension on the suture line and improve wound healing. |
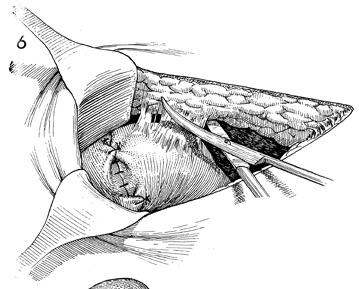
After the anastomosis is
completed, the peritoneum is entered, and adhesions are dissected
with Metzenbaum scissors. |
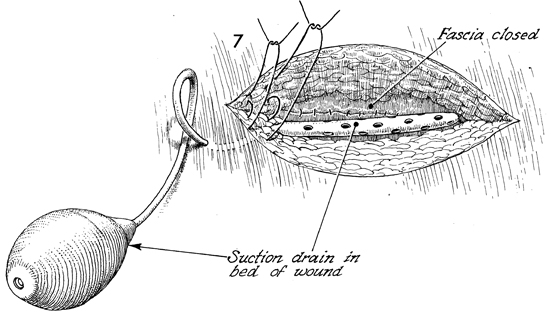
The rectus fascia has been closed with synthetic
delayed absorbable suture. A Hemovac suction drain is placed
above the closure of the fascia and below the subcutaneous tissue. |
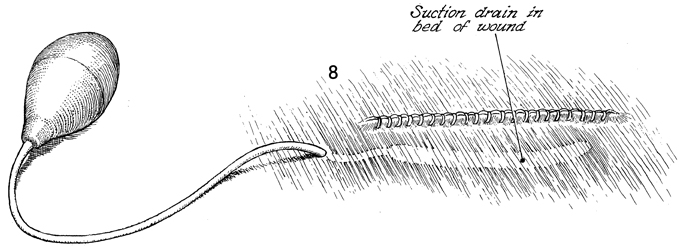
The skin is closed with stainless
steel clips. Note the suction drain ghosted under the closure.
This is removed in 24-36 hours. |
|
