
Colon
Appendectomy
Appendectomy
Using
the Linear Dissecting
Stapler
Transverse
Loop
Colostomy
End
Sigmoid Colostomy With Hartmann's Pouch
Closure
of a Loop
Colostomy
Anterior
Resection
of the Colon With Low
Anastomosis Using
the Gambee Suture
Technique
Low
Anastomosis
of Colon to Rectum
Using the End-to-End
Surgical Stapler
Technique
Anterior
Resection
of the Colon With
Low Anastomosis via
the Strasbourg-Baker
Technique |
Anterior Resection of the Colon
With Low Anastomosis Using
the Gambee Suture Technique
The purpose of this operation is to resect the rectosigmoid colon
and reanastomose the descending colon to the rectum by utilizing the
Gambee single-layer suture technique.
Physiologic Changes. The physiologic
changes associated with removal of the rectosigmoid colon are minimal.
If the patient has had total pelvic irradiation, a
low anastomosis should be protected by a temporary diverting colostomy
for 8-10 weeks. If there has been no pelvic irradiation and an adequate
preoperative bowel preparation has been performed, however, a diverting
colostomy may not be required.
Points of Caution. Adequate mobilization of the descending
colon, even if this means mobilizing the splenic flexure and transverse
colon, must be made in order that the descending colon will reach the
rectum without tension. Anastomoses performed under tension. Anastomoses
performed under tension do not heal well.
Technique
Two positions may be used for
this operation. First, if a simple anterior resection with low
anastomosis of the rectosigmoid colon is to be performed and
10-12 cm of rectum are to be preserved; the patient can be operated
on in the supine position. If there is a chance that the rectum
may require transection below 10 cm, however, the patient should
be operated on in the modified dorsal lithotomy position, exposing
the perineum for anastomosis using an EEA (end-to-end anastomosis)
stapler.
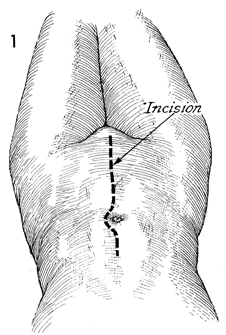
The abdomen, vagina, and perineum
should be surgically prepped prior to the procedure, and a Foley
catheter should be placed in the bladder. The abdomen should
be opened through a left paramedian or midline incision. |
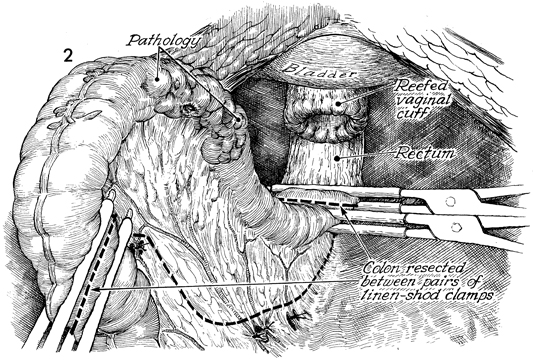
The diseased portion of the rectosigmoid
colon has been identified, and the appropriate segment of colon
has been selected for resection. Two linen-shod clamps are placed
at each end of the section designated. The surgeon clamps the
colonic vessels by opening small holes in the mesentery. If possible,
the left colonic branch of the inferior mesenteric artery is
preserved. The remaining portion of the mesentery is transected
with scissors. The colonic segment and its mesentery are removed. |
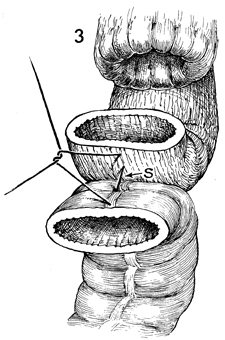
After the descending colon has been sufficiently
mobilized to allow approximation to the rectum without tension,
a stabilizing
3-0 synthetic absorbable suture
is placed at the mesenteric border (S) with a Lembert
stitch.
|
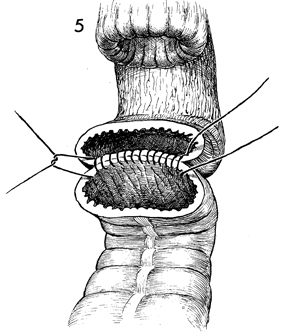
A Gambee through-and-through
single-layer anastomosis is begun with interrupted 3-0 synthetic
absorbable sutures. The needle is passed through the walls of
the rectum and descending colon, and each knot is tied on the
inside of the lumen (see Small Bowel
Resection With End-to-End Anastomosis Using the Gambee Technique). |
|
|
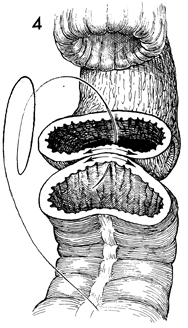
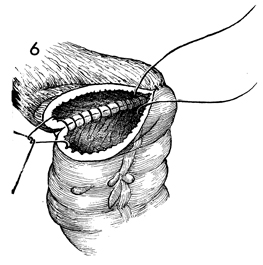
The
anastomosis is continued left and right around the circumference
of the lumen. |
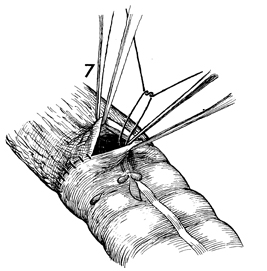
The last sutures in the antimesenteric
border of the bowel should be placed using a near-far inverting
stitch as demonstrated in Small Bowel
Resection With End-to-End Anastomosis Using the Gambee Technique. |
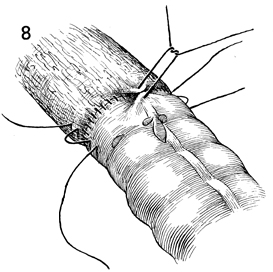
A few Lembert 3-0 synthetic absorbable sutures
are placed around the anastomosis to relieve tension. |
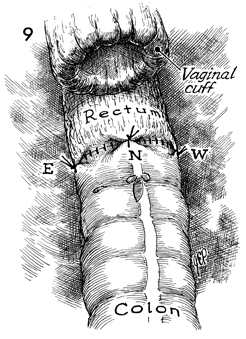
The anastomosis, completed with
Lembert tension-relieving sutures placed east (E), north
(N), and west (W) around the bowel, is shown.
Where the vaginal
cuff has been reefed following a hysterectomy is a convenient
site for insertion of a closed suction drain.
A Salem pump nasogastric tube
is placed in the stomach and connected to low suction until bowel
function is established. |
|
|
