|
||||||
Small
Bowel Resection Small
Bowel Bypass Small
Bowel Bypass Terminal
Ileectomy |
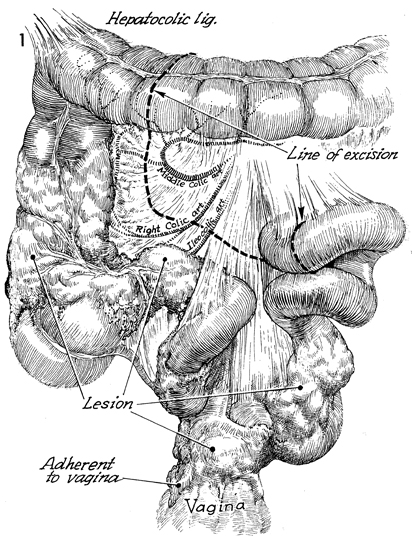
Terminal
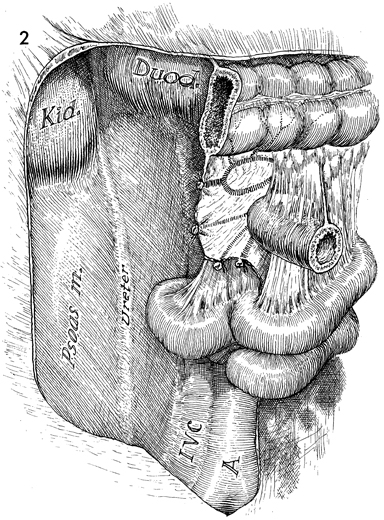
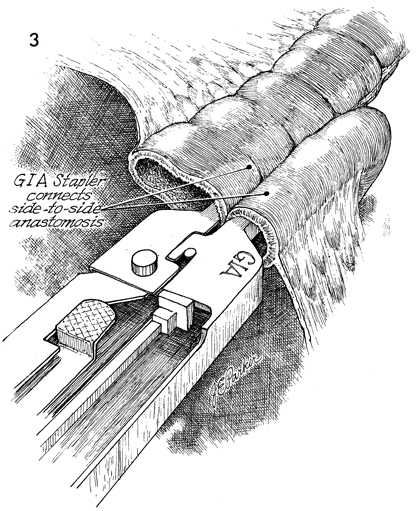
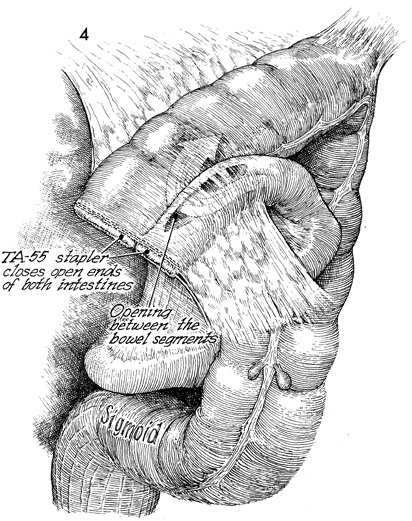
Ileectomy With Right The presence of a tumor or severe irradiation damage to the terminal ileum and right colon, with or without obstruction, may require resection of the affected area. Physiologic Changes. Resection of a portion of the terminal ileum is associated with a loss of absorption of the fat-soluble vitamins A, D, C, and K. Vitamin B12 is normally absorbed in the terminal ileum; thus when the terminal ileum is absent B12 must be given systemically. Loss of the terminal ileum creates changes in cholesterol metabolism and bowel salt reabsorption. If undigested fats are dumped directly into the transverse colon, the osmotic pressure of the colon is elevated, and diarrhea results. Points of Caution. After the abdomen has been opened through a midline incision extended to the xiphoid, care should be taken to identify the blood supply to the right colon and terminal ileum. If at all possible, the colon should be transected distal to the middle colic artery. The ileocolic artery frequently has to be clamped and tied. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.