|
||||||||||
Insertion of Suprapubic Catheter Retropubic
Urethropexy: Ureteroneocystostomy Transperitoneal Intestinal
Loop |
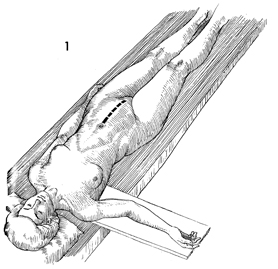
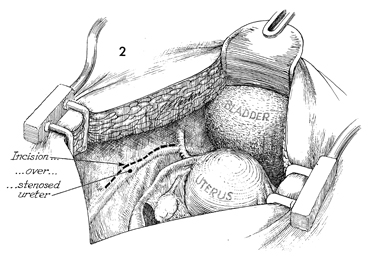
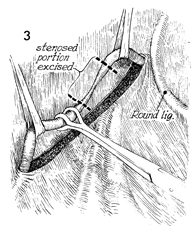
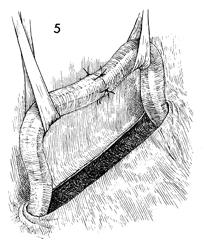
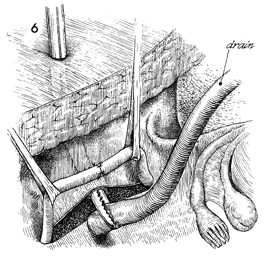
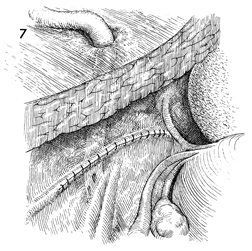
Ureteroureterostomy Injury to the ureter is occasionally high enough in the pelvis for a primary ureteroureterostomy to be performed without having to resort to a ureteroneocystostomy. In these cases, the ureter has been damaged at or near the pelvic brim while clamping, incising, and ligating the infundibulopelvic ligament or while excising an extensive ovarian carcinoma that has distorted the pelvic anatomy at or near the pelvic brim. Although less common than procedures for correcting lower injuries to the ureter, a ureteroureterostomy is preferable to a ureteroneocystostomy when it can be performed without tension on the anastomosis producing the stenosis. The essential features of the procedure are the adequate mobilization of the cut ends of the ureter to prevent tension on the anastomosis, the use of a spatulated anastomosis, and the use of delicate suture, meticulous hemostasis, and drainage of the anastomosis site via a closed suction drain through the lower abdominal wall. The purpose of the ureteroureterostomy is to anastomose the transected ureter. Physiologic Changes. After a damaged or diseased portion of the ureter has been removed, the ureter is anastomosed. The sequelae of ureteral obstruction and/or laceration are relieved. Points of Caution. Care should be taken to see that
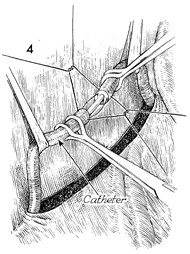
the ureter is anastomosed without tension. A soft Silastic indwelling catheter should be placed through the anastomotic area and fed into the bladder caudad and the renal pelvis cephalad. The drain should be placed in the area of the anastomosis and brought out through the right or left lower quadrant and kept in place until all external drainage has ceased. Technique
|
|||||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.