
Bladder
and Ureter
Insertion
of Suprapubic Catheter
Retropubic
Urethropexy:
Marshall-Marchetti-Krantz
and Burch Operations
Ureteroureterostomy
Ureteroneocystostomy
and Ureteroneocystostomy
With Bladder Flap
Transperitoneal
Ureteroureterostom
End-to-Side Anastomosis
Intestinal
Loop
Urinary Diversion
Percutaneous
Nephropyelostomy
Ureteroileoneocystostomy
Clam
Gastrocystoplasty |
Transperitoneal Ureteroureterostomy
(End-to-Side Anastomosis)
In some patients, resection of the terminal ureter
is required for complete removal of a pelvic malignancy. In these cases,
diversion of the urine must be achieved by either ureteroneocystostomy
or transperitoneal ureteroureterostomy.
If the opposite ureter is normal
and healthy and if there is any sizeable distance between the damaged
ureter and the bladder, transperitoneal ureteroureterostomy is preferred.
Postoperative stricture formation following ureteroneocystostomy is
frequently produced by tension on the anastomotic suture line. Therefore,
in these cases, end-to-side transperitoneal ureteroureterostomy may
allow a tension-free anastomosis.
In those cases associated with pelvic irradiation, transperitoneal
ureteroureterostomy allows diversion of the urine at a site outside
the fields of irradiation without tension, thus avoiding the problem
of stenosis in a surgical anastomosis within heavily irradiated tissue.
The
basic concept of transperitoneal ureteroureterostomy is to bring the
ureter from one side across the peritoneal cavity under the mesentery
of the intestine to the healthy ureter on the opposite side and to
anastomose it. We prefer to perform all of these anastomoses over a
Silastic catheter stent that is left in place for approximately 2 weeks.
The
purpose of the operation is to save the kidney, when its ureter has
been injured or obstructed, by implanting that ureter in a healthy
ureter on the opposite side to allow the free flow of urine from both
kidneys through one ureter to the bladder.
Physiologic Changes. If stricture is avoided at the
anastomotic site and if there is no obstruction to the terminal portion
of the recipient ureter, few if any physiologic changes occur. A single
ureter is capable of carrying the entire flow of urine from both kidneys.
If the disease process has obstructed the ureter on one side, however,
it may eventually obstruct the ureter on the opposite side, thus requiring
a second diversion by ileal loop.
Points of Caution. Care should be
taken to excise the damaged portion of the injured ureter. The affected
ureter should be handled in a delicate manner to avoid damaging the
network of vessels under the ureteral sheath that provides the blood
supply to the ureter from the renal pelvis to the bladder. A 1 x 1/2
cm segment of the wall in the recipient ureter is removed for the anastomosis
rather than making an incision into the ureter for the anastomosis.
This, we feel, reduces the incidence of postoperative stricture formation.
We prefer (1) to spatulate all ureteral anastomoses to prevent iris
contracture and (2) to perform the anastomosis over a Silastic tube
stent. The site of the anastomosis should be drained retroperitoneally
through the lower quadrant by a closed suction drain.
Technique
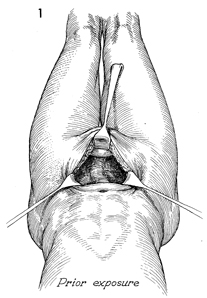
The patient is placed on the operating table
in the dorsal supine lithotomy position. A Foley catheter has
been placed in the bladder. The abdomen is opened through a lower
midline incision. |
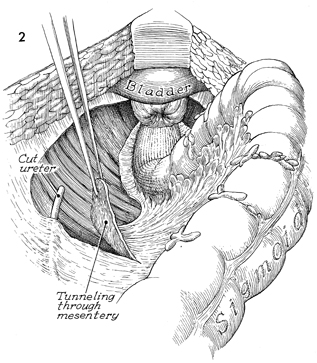
The peritoneum over the common iliac vessels
of the affected side is elevated and opened with Metzenbaum scissors,
exposing the entire path of the diseased or damaged ureter. The
diseased portion of the ureter is identified. The distal segment
of ureter going to the bladder is cross-clamped and tied with
a 0 synthetic absorbable suture. The proximal segment of the
ureter for implantation is carefully mobilized, preserving the
blood supply by preventing damage to the ureteral sheath and
the underlying network of vessels. All damaged portions of the
ureter should be removed, and in cases of pelvic irradiation,
the entire irradiated portion of the ureter should be removed.
The peritoneum covering the mesentery of the large bowel is opened,
and a tunnel is created under the mesentery. Care is taken to
prevent damage to the vessels in the mesentery of the large bowel. |
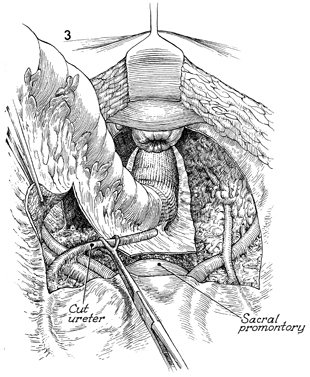
The damaged ureter is brought through the
tunnel in the mesentery of the large bowel. The peritoneum overlying
the common iliac artery on the opposite side is elevated and
opened. The healthy ureter is identified and dissected for an
appropriate distance. |
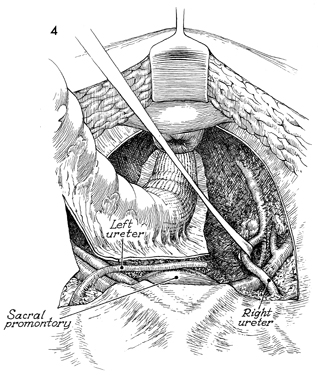
The recipient ureter is elevated with a vein
retractor. The ureter to be implanted is brought adjacent to
the recipient ureter at a convenient site. Extreme care should
be taken at this point to ensure that there is proper mobility
and that there will be no tension on the suture line. The damaged
ureter should be brought to the normal ureter. The normal ureter
should be mobilized only enough to perform the anastomosis. |
We prefer to perform all ureteral anastomoses
over a Silastic tube stent. It is difficult to insert a flexible
Silastic tube stent down the recipient ureter into the bladder.
Therefore, we have evolved the following technique to bring a
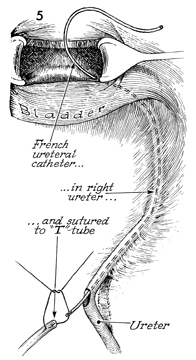
flexible Silastic tube into the bladder. A cystotomy is performed,
and a No. 5 French whistle-tip ureteral catheter is inserted
through the ureteral orifice up the recipient ureter to the area
of ureterotomy. The No. 5 French whistle-tip ureteral catheter
is passed through the defect in the recipient ureter and sutured
to the Silastic T-tube with a 4-0 Prolene suture. |
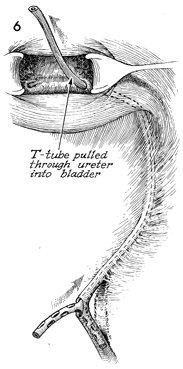
The Silastic tube stent is
then pulled through the distal ureter with the ureteral catheter
into the bladder. The arms of the T-tube are passed into the
recipient and the implanted ureters. |
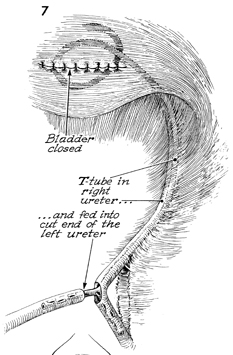
The Silastic T-tube is coiled in the bladder.
The cystotomy in the bladder is closed in two layers with 3-0
synthetic absorbable suture. The second arm of the T-tube is
fed into the ureter to be implanted. |
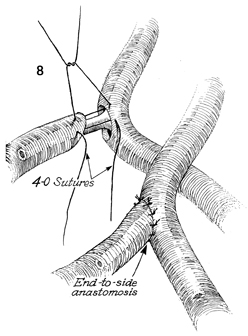
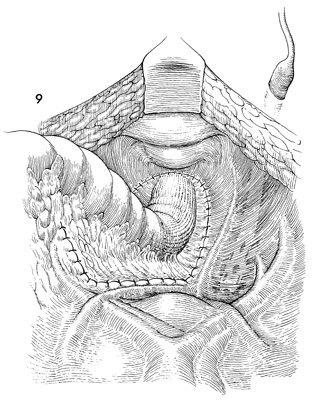
The ureteroureterostomy end-to-side
anastomosis is performed with interrupted 4-0 synthetic absorbable
sutures in a through-and-through technique, creating a mucosa-to-mucosa
anastomosis. A spatulated ureteral anastomosis is less likely
to develop an iris contracture. |
The peritoneum is closed over the ureteral
anastomosis. A closed suction drain is placed through the lower
quadrant of the abdomen and brought retroperitoneally up to the
site of the ureteroureterostomy. It is left in place until drainage
ceases. A water cystoscopy is performed 2-3 weeks postoperatively,
and the Silastic T-tube stent is removed. An intravenous pyelogram
(IVP) is performed at that time and repeated every 2 months until
the surgeon is satisfied with the results of the anastomosis. |
|
|
