
Bladder
and Ureter
Insertion
of Suprapubic Catheter
Retropubic
Urethropexy:
Marshall-Marchetti-Krantz
and Burch Operations
Ureteroureterostomy
Ureteroneocystostomy
and Ureteroneocystostomy
With Bladder Flap
Transperitoneal
Ureteroureterostom
End-to-Side Anastomosis
Intestinal
Loop
Urinary Diversion
Percutaneous
Nephropyelostomy
Ureteroileoneocystostomy
Clam
Gastrocystoplasty |
Intestinal
Loop Urinary Diversion
There are several ways in which the urinary
system can be diverted: nephrostomy, cutaneous ureterostomy, ureterosigmoidostomy,
intestinal loop urinary diversion, and continent urostomy. Intestinal
loop is a good procedure for diverting the urine in elderly patients
or in patients without sufficient bowel to perform one of the continent
urostomies. This procedure began as an ileal loop urinary diversion.
The colon loop urinary diversion eliminates the need for a bowel resection
in the terminal ileum. This is particularly important when the patient
has had total pelvic irradiation. Hyperchloremic
acidosis associated with implantation of the ureters into the intact
sigmoid colon does not occur with colon loop urinary diversion because
the average length of the colon loop, 8-10 cm, is too short for significant
absorption of urine from the colonic mucosa.
The purpose of the intestinal loop
urinary diversion is to divert the urine following removal of the bladder
at the time of anterior or total exenteration or if the bladder and
lower ureters have lost their neurologic function and a continent urostomy
is contraindicated.
Physiologic Changes. The most significant physiologic
change of an intestinal loop urinary diversion is the rapid runoff
of urine from the isolated intestinal loop.
Because of this, the incidence
of urinary tract infection is less than that encountered when the ureter
is implanted into a functional segment of the rectosigmoid colon.
A
negative change in intestinal loop diversion is the problem of contaminated
reflux from the loop of the renal pelvis. This produces loss of upper
renal units in 65% of patients.
Points of Caution. The ureters should
be transected as low in the pelvis as possible. Excess ureter can be
trimmed away if necessary. Silastic catheters should always be inserted
up the ureter and through the intestinal loop to splint the anastomosis
for 10-12 days. This alone has significantly reduced the incidence
of ureteral stricture and separation from the intestinal anastomotic
site.
Another point of caution concerns the design of the
loop. In general, it should be selected from bowel that has had the
least irradiation. The length should be long enough to reach the abdominal
wall, usually 8-12 cm. Care should be taken to close mesenteric defects
in the reanastomosed intestine and those between the loop and the abdominal
side wall to prevent internal hernia.
Techniques
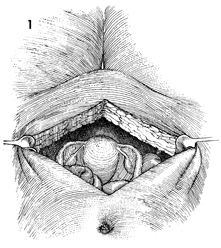
The patient is placed in the supine position,
and the abdomen is opened through a lower midline incision. Occasionally,
extension of the incision around the umbilicus is required. The
pelvis is thoroughly explored, and both ureters are identified
and traced as deep in the pelvis as is technically possible. |
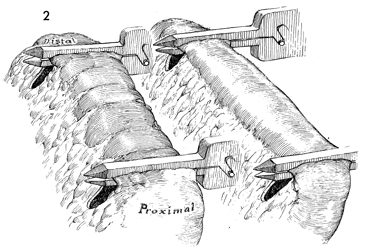
The loop of bowel to be used, colon or ileum,
is selected. Figure 2 shows the terminal ileum and the colon.
The appropriate length of bowel is measured, selected, and marked.
The mesentery of the bowel is carefully illuminated with bright
light to delineate the vascular arcades. This confirms that the
loop is adequately nourished by a generous blood supply from
the vascular branches of the arcade. The mesentery of the loop
is opened for approximately 4-5 cm, and the small vessels are
clamped and tied. The loop can be transected in the classic way
between Kocher clamps. Today, however, the automatic surgical
stapler with TA-55 premium absorbable staples for the proximal
end of the loop is often used. If wire or permanent suture is
used in the proximal end of the loop, stone formation may occur.
As shown here, a GIA (gastrointestinal
anastomosis) stapling and division device can be applied to the
distal portion of the loop. A standard TA-55 wire staple can
be applied to the proximal portion of the bowel, but a TA-55
premium absorbable staple is preferable for the proximal portion
of the loop. If staples are not available, the proximal loop
can be closed with synthetic absorbable suture.
After all of these staples
are fired, the loop can be transected between the TA-55 wire
staples and the TA-55 absorbable staples. A standard bowel anastomosis
can be made between the proximal and distal ileum or proximal and
distal colon as outlined in the technique in Figure 7-10. |
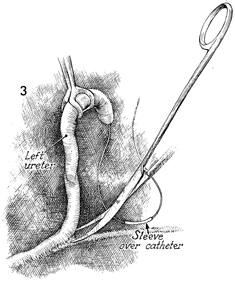
The ureter is identified deep
in the pelvis and mobilized, presevering the delicate ureteral
sheath that surrounds the ureter from the renal pelvis to the
bladder. After transecting the ureter, the distal stump is tied
with 0 synthetic absorbable suture. The proximal ureter is catheterized
with a Silastic "J" ureteral anastomosis catheter that contains
either a suture sleeve or a suture rib.
If the ileal segment
of bowel has been selected, the mesentery of the rectosigmoid
colon must be opened to allow the left ureter to be transported
through the mesentery to bring it into position for anastomosis
to the ileum. If the sigmoid colon has been selected for the
loop, this is not necessary, since the mesentery will already
be open. |
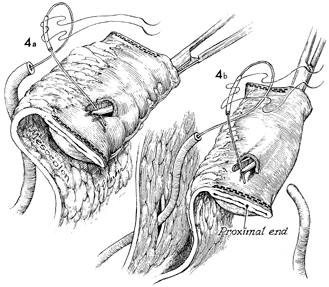
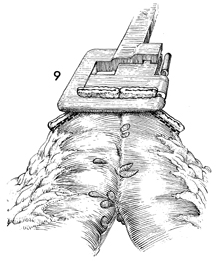
The intestinal segment has been cross-clamped
with the GIA stapler, so that both proximal and distal ends of
the segment are stapled closed. A small opening must be made
in the distal segment of the loop to admit a narrow arterial
forceps that is advanced down the segment of bowel to within
3 cm of the distal end. At that point, the arterial forceps is
slightly elevated, and an incision is made over the tip of the
arterial forceps until the intestine is entered. A small button
of bowel wall measuring 1 x 1 cm in diameter may be removed.
The forceps is advanced through this opening and grasps the Silastic
catheter that is in the ureter. A 4-0 synthetic absorbable suture
on two small needles has been previously placed through the Silastic
suture sleeve or suture rib on the Silastic catheter.
If an ileal
segment of bowel is to be used as seen in b,
a defect has to be created in the mesentery of the sigmoid colon
to allow the left ureter to be brought through that defect and
into position for an anastomosis to the ileum. In b,
the right ureter is seen in the approximate position for anastomosis. |
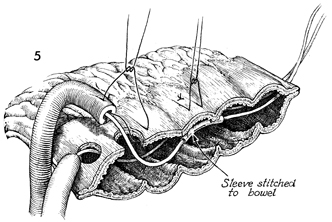
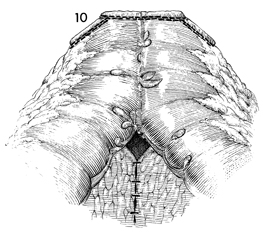
This sagittal section of the
intestinal segment illustrates the technique of suturing the
Silastic catheter sleeve with a fine 4-0 synthetic absorbable
suture to the wall of the intestine to hold the Silastic catheter
in place and prevent peristalsis of the ureter from pushing the
catheter into the loop and thus out of the ureter. This step
is unnecessary if the stent has a "J" or "pigtail" configuration
that prevents expulsion. The Silastic catheter should stay in
the ureter, stenting the anastomosis, for at least 10-12 days.
The sutures for the ureteral intestinal anastomosis are placed
full thickness through the bowel wall and the ureter so that,
when tied, a mucosa-to-mucosa anastomosis is performed. |
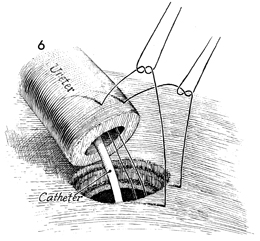
The ureter is anastomosed
to the intestinal wall with interrupted 4-0 synthetic absorbable
sutures. Generally, 4-5 sutures are needed to complete the anastomosis.
In addition, some periureteral peritoneum is anchored across
the anastomosis to take tension off the suture line. The opposite
ureter is sutured to the intestine in a similar manner. |
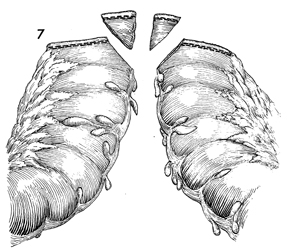
The intestinal segments are lifted superior
to the constructed loop, allowing an end-to-end functional anastomosis
to be completed between the segments of bowel. If a segment of
rectosigmoid colon is used, the intestinal loop is moved medially
to allow an end-to-end colocolostomy.
Figure 7 shows the anastomosis being performed
on the descending colon, but the technique of the stapler anastomosis
is the same for both large and small bowel. |
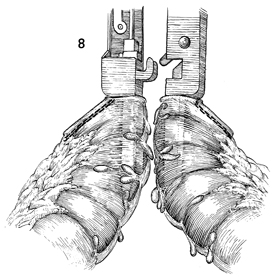
Both blades of the GIA stapler
are passed into the colon along the antimesenteric border. The
stapler is activated, and a V-shaped ostium is created along
the antimesenteric border for a distance of approximately
5 cm with a double row of staples on each side and an incision
down the middle. |
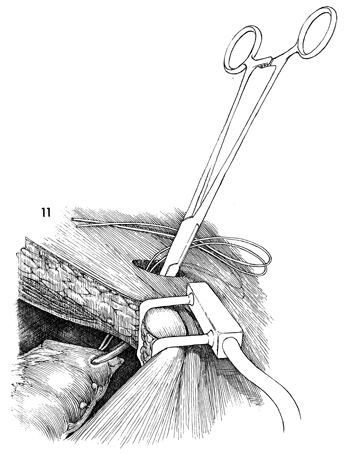
The edges of the remaining defect are picked
up with Babcock clamps and brought through the activated TA-55
stapler. Any excess bowel is trimmed away with curved Mayo scissors. |
The functional end-to-end anastomosis is
completed. The mesentery is sutured with interrupted 3-0 synthetic
absorbable sutures. |
The distal portion of the intestinal urinary
loop, with the ureters anastomosed in place, is pulled through
the abdominal wall defect, which should be at least 2 fingersbreadth
or 4 cm in diameter. The excess Silastic catheter is trimmed
away. |
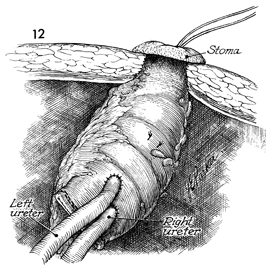
The stoma is sutured to the
skin of the abdominal wall with a rosebud stitch, as shown in
the operation for end sigmoid colostomy (see Colon), which raises
the stoma approximately 1 cm above the level of the skin and
allows urine to drip off the stroma into its bag without contact
with the skin. The mesentery of the intestinal segment must be
carefully closed to the lateral pelvic wall to prevent internal
hernia. |
|
