|
||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
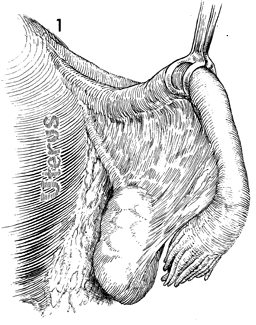
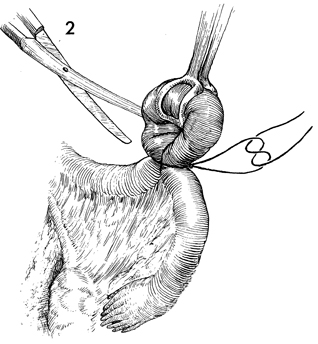
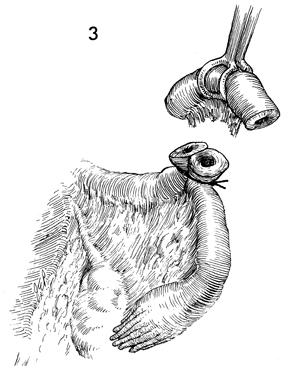
Sterilization by the Pomeroy Operation The Pomeroy operation is the most popular and widespread operation performed for female sterilization. It can be performed postpartum, at the time of cesarean section, or at interval sterilization through either mini-laparotomy or vaginal colpotomy. The purpose of the operation is to obstruct the female Fallopian tubes and prevent pregnancy. Physiologic Changes. All methods of tubal sterilization have a reported incidence of menometrorrhagia. This varies with different series. The exact physiologic changes that produce menometrorrhagia are unknown at this time. The theory that ligation of the Fallopian tube reduces or alters ovarian blood supply remains to be proven. Points of Caution. A 0 synthetic absorbable suture is preferable to permanent suture for ligating the knuckle of Fallopian tube. If the two ends of the Fallopian tube are permanently held in approximation, there may be a greater chance of recanalization than if they are allowed to separate when the suture is absorbed. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.