|
||||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
Sterilization by the Minilaparotomy is ideal for thin women with no pelvic disease or adhesions.
The procedure is difficult to perform in obese women or in women who
have had inflammatory disease of the Fallopian tubes. In thin, small patients it has the advantage of being
performed with instruments less costly than those for laparoscopy.
When the patients are given a choice, however, they usually prefer
laparoscopy because recovery is faster and less painful and they can
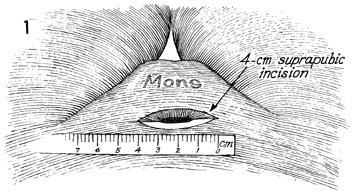
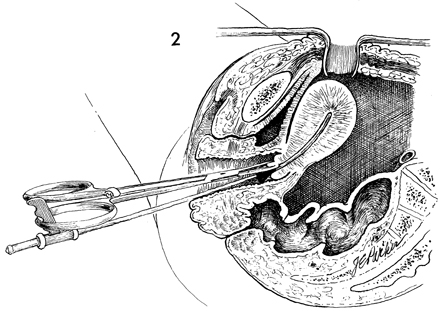
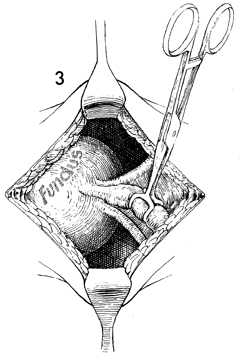
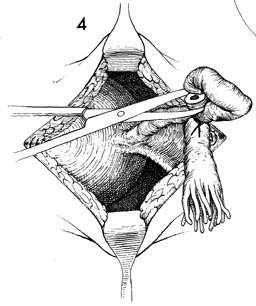
resume their activities much sooner. The purpose of the procedure is to obstruct the Fallopian tubes. Physiologic Changes. The Fallopian tubes are obstructed. Points of Caution. The bladder must be empty, or cystotomy can result. If more than 4 cm are needed to enter the abdomen - the width of 2 adult fingers - the patient is too obese for this operation, and a laparotomy should be performed with the patient under general anesthesia. Technique
|
|||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.