
![]()
Insertion of Suprapubic Catheter
Retropubic Urethropexy: Marshall-Marchetti-Krantz and Burch Operations
Ureteroneocystostomy and Ureteroneocystostomy With Bladder Flap
Transperitoneal Ureteroureterostom End-to-Side Anastomosis
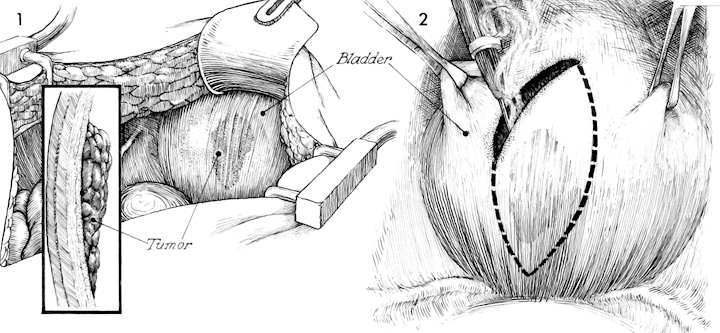
Wedge Resection of Bladder
Open cystotomy and intravesicle inspection of the urinary bladder is a useful procedure in many circumstances. The wedge resection (removal of a section of bladder) is used to remove isolated small bladder tumors. In many patients so treated, additional therapy with pelvic irradiation is needed to control small malignant tumors.
The purpose of the procedure is to remove a diseased segment of the bladder wall while maintaining the remainder of the bladder for urinary function.
Pathophysiologic Changes: As much as 40% of the bladder can be removed without producing extreme frequency of urination or significant reduction in bladder capacity.
Points of Caution: The pathway of the ureter must be identified before resecting the bladder. If in doubt, preoperative catheterization of the ureters can be performed so that the ureters can be palpated and seen after cystotomy. If preoperative catheterization of the ureters has not been performed and the ureteral orifice or the intravesicle portion of the ureter might be compromised by the resection, a ureteral catheter should be passed at the time of cystotomy.
A closed suction drain should always be placed in the area of closure in the urinary tract. It should be kept in place until drainage has ceased.
Technique
With the patient in the dorsal position the abdomen is prepped, draped, and opened through a lower midline incision.
After the abdomen had been adequately explored for extension of the disease to the upper abdomen, the intestine is packed away and the bladder is exposed. Frequently, the pathologic area can be palpated through the bladder wall. The vesicle-abdominal peritoneum can be retracted and the space of Retzius opened.
The initial incision is made into the dome of the bladder through the space of Retzius in the retroperitoneal area. The dome of the bladder is picked up with two Allis clamps and placed on retraction. The electrocautery scalpel is used to open a cystotomy site through which a finger can be inserted. The incision can be expanded by blunt dissection. Use of the cautery scalpel and blunt dissection appears to reduce bleeding. Small bladder wall blood vessels should be clamped and electrocoagulated. If they are to be tied, they should be tied with a synthetic absorbable suture, as permanent suture placed in this area can lead to stone formation. The outline of the area of resection is made with brilliant green.
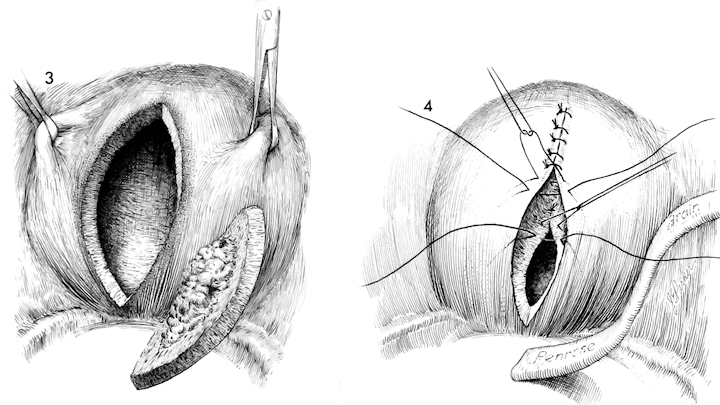
The outlined section along with a wide margin of normal tissue is removed.
The bladder is closed in layers with interrupted 3/0 synthetic absorbable suture, the first layer on the mucosa, the second layer on the muscularis and peritoneum. A closed suction drain is placed into this space and brought out through the lower quadrant of the abdomen. It should not be removed until all urinary drainage has ceased.