
Cervix
Biopsy
of the Cervix
Directed
Biopsy of the Cervix at Colposcopy
Endocervical
Curettage
at Colposcopy
Conization
of the
Cervix by the Loop Electrical Excision Procedure (LEEP)
Cryosurgery of Cervix
Conization of Cervix
Abdominal
Excision
of the Cervix Stump
Correction
of an Incompetent Cervix
by the Shirodkar
Technique
Correction
of an Incompetent Cervix
by the McDonald
Operation
Correction
of an Incompetent Cervix
by the Lash Operation |
Conization of the Cervix
by the Loop Electrical Excision
Procedure (LEEP)
The indication for conization of the cervix are (1)
the limits of the lesion in the cervix cannot be completely defined
by colposcopy and directed biopsy, or the lesion is noted to extend
up into the cervical canal and, therefore, is inaccessible to histologic
examination by direct biopsy; (2) there is severe cervical intraepithelial
neoplasia (CIN) or carcinoma in situ in a young patient for whom a
hysterectomy is contraindicated because of age and desire for fertility;
and (3) there is a failure of agreement between cytology, colposcopy,
and histology. The purpose of conization of the cervix by the LEEP
is to remove a cone-shaped piece of cervical tissue that will encompass
the squamocolumnar junction. The procedure can be diagnostic as well
as therapeutic.
Physiologic Changes. This operation removes the endocervical
glands and in some patients has been associated with infertility because
it reduces the production of cervical mucus. In addition, it may weaken
the internal os of the cervix and, therefore, can be associated with
second-trimester abortion.
Points of Caution. The surgical
specimen should be adequate to provide an accurate diagnosis and
remove the entire lesion. Hemostasis after conization is essential.
These patients should be informed that there may be a small incidence
of persistent cervical intraepithelial neoplasia following conization
by the LEEP. Therefore, follow-up cytology and colposcopy are essential
to this form of therapy.
Technique
The patient may be anesthetized
with general or local anesthesia. Local anesthesia consists of
paracervical injections of 1% lidocaine at the 3, 5, 7, and 9
o'clock positions around the cervix. The cervix is stained with
an iodine solution such as Schiller's solution to demarcate zones
of glycogen depletion and thus neoplasia. If the patient is under
general anesthesia, a solution of Pitressin diluted with 10 international
units to 30 mL of normal saline is injected around the entire
surface of the cervix. If the patient is under local anesthesia,
the Pitressin can be mixed with lidocaine. Vascular constricture
and blanching of the cervix will be noted. The injection of Pitressin
solution is contraindicated in patients with cardiovascular disease
and /or hypertension. A pursestring vascular cerclage to control
the bleeding is rarely indicated. |
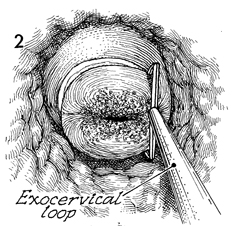
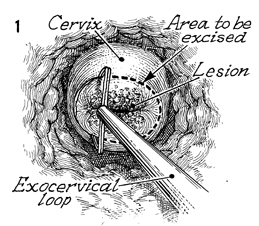
With the lesion adequately stained
with Schiller's solution, the loop device with suction attached
to the rod removes the smoke or flume. The loop is placed outside
the lesion in the area of normal cervix. The electrocoagulator
is adjusted to a blend between the cutting and the electrocoagulation
current. The loop device is inserted through the cervical tissue
to the depth of the available loop and is slowly moved from one
side of the portio of the cervix to the other side. By inserting
the loop to the full depth of the cervix, the cone should contain
the entire lesion. When the surgeon has reached the opposite
limits of the lesion as noted by Schiller's white area, the loop
is lifted forward, and the specimen is removed. |
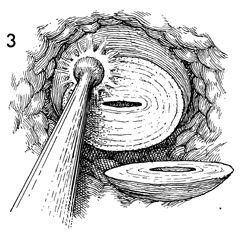
Electrocoagulation of any bleeding surfaces
with the ball cautery is performed. |
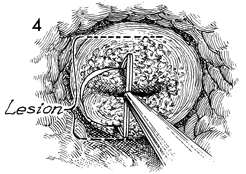
The lesion is larger than (extends outside
the limits of) the available steel loops and must be removed
in sections (see Figs. 5-8). The electric wire of the loop is
inserted and swept across the cervix in a routine fashion as
shown in Figures 1-3. |
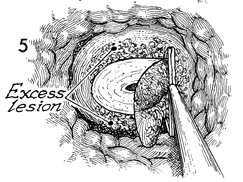
Excessive lesion remains outside that removed
by the LEEP. |
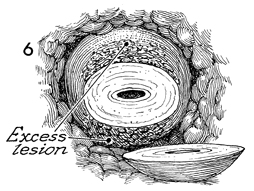
The cone is removed, but
excessive lesion can still be seen outside the excised area. |
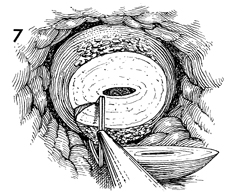
The remaining lesion can be removed by repeating
the standard procedure, moving the electrical loop from one side
to the other. The lesion that was outside the original cone has
been removed. |
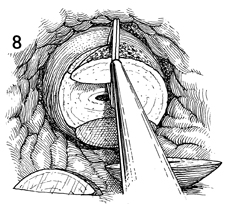
The lesion on the anterior
lip of the cervix is removed in a similar manner. |
The three cone specimens of the cervix are
removed by LEEP are (1) the original cone, (2) the posterior
portion, and (3) the anterior portion. |
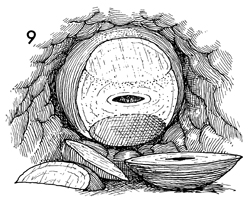
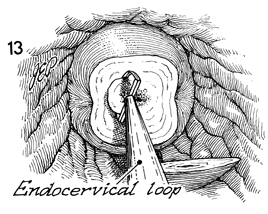
When the original lesion extends
high into the endocervical canal, the cone specimen of the cervix
is removed as shown here. Conization by the LEEP is moved from
the patient's right to the left in the same technique as previously
shown. |
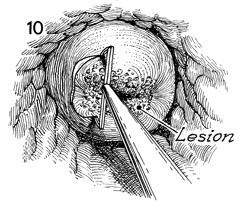
Most of the lesion has been removed by the
LEEP. |
The exterior lesion on the portio is completely
removed, but neoplasia remains in the cervical canal. |
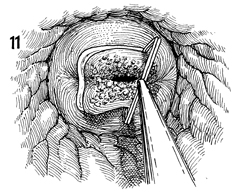
A smaller loop is placed up the canal. The
remaining portion of the endocervical canal is removed by LEEP. |
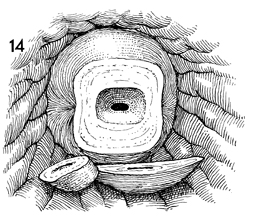
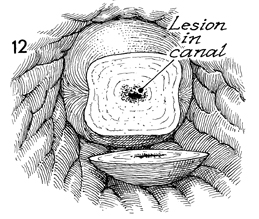
The two pathologic specimens, the cylinder
and the cone, are shown here. Hemostasis can be achieved as shown
in Figure 3 by the ball cautery. The specimens are sent to pathology
clearly marked as upper cervical canal and lower squamous columnar
junction of the cervix.
We have found it advantageous
to dip a tampon in a ferrous sulfate solution such as Monsel's.
The tampon with the tip soaked in Monsel's solution is placed
in the cervical cone for additional hemostasis. |
|
