
Cervix
Biopsy
of the Cervix
Directed
Biopsy of the Cervix at Colposcopy
Endocervical
Curettage
at Colposcopy
Conization
of the
Cervix by the Loop Electrical Excision Procedure (LEEP)
Cryosurgery of Cervix
Conization of Cervix
Abdominal
Excision
of the Cervix Stump
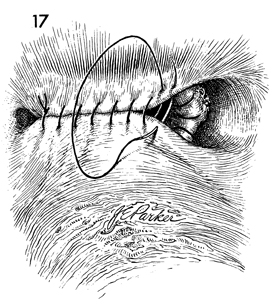
Correction
of an Incompetent Cervix
by the Shirodkar
Technique
Correction
of an Incompetent Cervix
by the McDonald
Operation
Correction
of an Incompetent Cervix
by the Lash Operation |
Abdominal Excision
of the Cervical Stump
Fortunately, subtotal abdominal hysterectomy is a relatively
rare procedure today. The pelvic surgeon may, however, encounter a
patient who underwent this operation in the past and has developed
neoplasia or myoma in the cervical stump. In such cases, surgery is
indicated.
Care should be exercised in removal of the stump.
The bladder and/or the rectum may have been used to reestablish the
peritoneal lining of the pelvis after the subtotal abdominal hysterectomy.
Therefore, these organs may be injured during the resection.
The transverse
incision is useful in those conditions where overall abdominal exploration
and exposure are not needed. The vaginal cuff is left open for drainage
to reduce the incidence of postoperative pelvic infection and abscess.
The
purpose of this operation is to remove the cervical stump via the abdominal
route.
Physiologic Changes. The diseased cervix is removed.
Points of Caution. Because of previous surgery, the
ureters may be densely adherent to the cervical stump. Care must be
taken to properly identify these and to free them both laterally and
vertically during the dissection of the bladder from the cervix.
Technique
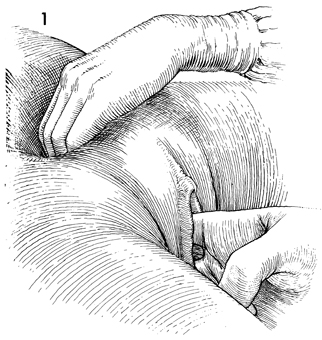
The patient is examined under anesthesia.
At this time, the vagina and abdomen should be surgically prepped,
and a Foley catheter should be inserted into the bladder and
connected to straight drainage. |
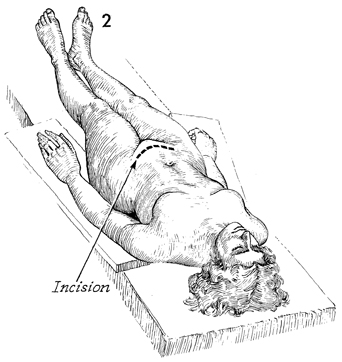
The patient is placed in the supine position,
and a transverse incision 12-14 cm in length is made following
the skin lines above the mons pubis. By keeping the incision
slightly above the mons pubis, the surgeon can avoid the vascular
plexus within the mons and aid hemostasis. |
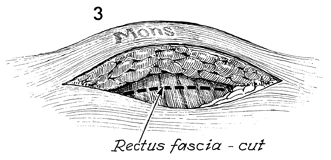
The incision is carried down to the rectus
fascia, which is incised transversely, exposing the rectus abdominal
muscles. |
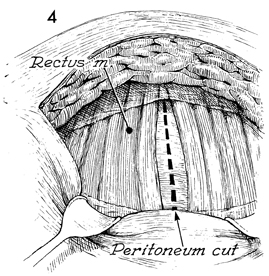
The rectus abdominal muscles can be separated
in the midline, and greater exposure can be achieved by undermining
the rectus abdominal muscles lateral to the inferior epigastric
artery. If greater mobility is required or if the rectus muscle
needs transection, the inferior epigastric artery and vein should
be ligated prior to extensive mobilization and/or muscle transection.
The peritoneum is elevated and can be opened in the transverse
or longitudinal plane. |
A self-retaining retractor is
placed in the incision. The pelvis and abdomen are explored.
The patient is placed in the moderate Trendelenburg position,
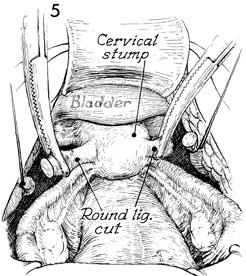
and the bowel is packed off with wet, warm gauze packs. Frequently,
the bladder peritoneum has been closed over the cervical stump,
and the only recognizable structures are (1) the round ligaments
as they enter the pelvic wall and (2) the tubes and ovaries.
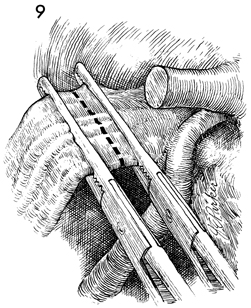
The round ligaments should be identified first, elevated with
an Ochsner clamp and suture ligated. By elevating the transected
round ligament, a plane of dissection can be achieved that in
most cases will allow the surgeon to free the bladder from the
cervix. The round ligaments in these cases have generally been
sutured back to the cervical stump and, therefore, appear to
be originating from the upper lateral area of the cervical stump.
The tube and suspensory ligament of the ovary are frequently
involved in the attachment to the cervical stump; and to avoid
hemorrhage, these structures should not be cut. |
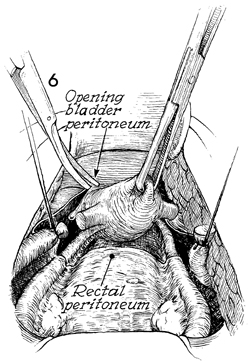
With adequate elevation of
the cervical stump via the round ligaments, the anterior leaf
of the broad ligaments can be identified. Sharp dissection is
used to incise the bladder peritoneum as well as the posterior
leaf of the broad ligament and the peritoneum overlying the cul-de-sac
and the rectum. |
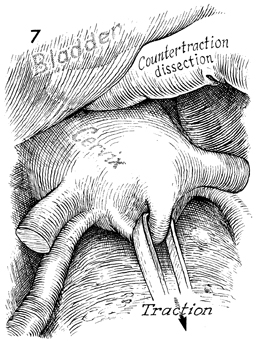
By elevating the bladder and vesical peritoneum
with the bladder blade of the retractor, the filmy attachments
of the bladder to the cervix can be identified and taken down
with blunt or sharp dissection. This is facilitated by placing
cephalad retraction on the cervical stump. |
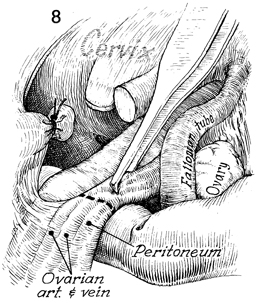
If the tubes and ovaries
remain, it may be advisable to remove them by identifying the
infundibulopelvic ligament and undermining the ligament with
the ovarian artery and vein below the brim of the pelvis. Care
at this point should be taken to identify the ureter, since,
as a result of previous scarring, it may have been diverted into
the general field of the infundibulopelvic ligament and, therefore,
be accessible to damage. |
The infundibulopelvic ligament should be
doubly clamped with Ochsner clamps and transected. |
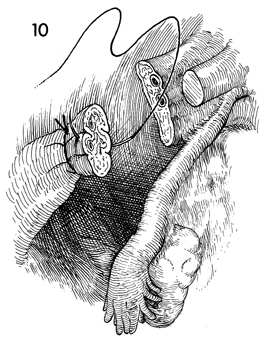
Two ligatures are customarily applied to
the stump of the infundibulopelvic ligaments: a tie of 2-0 synthetic
absorbable suture and a suture placed through the midportion
of the stump and tied to both sides. |
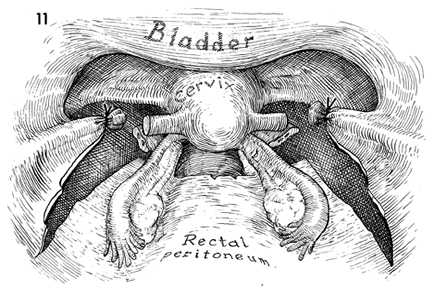
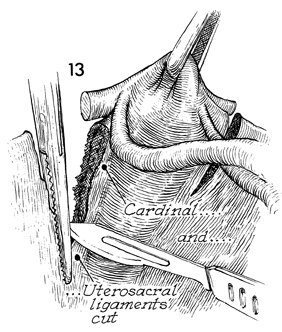
The cervical stump has now been
freed form the round ligament and infundibulopelvic ligament.
The peritoneum has been opened with a 360° arch around
the cervical stump. The upper portions of the cardinal ligaments
have been clamped and tied. The remaining cardinal ligaments
and uretrosacral ligaments remain to be cut and tied. |
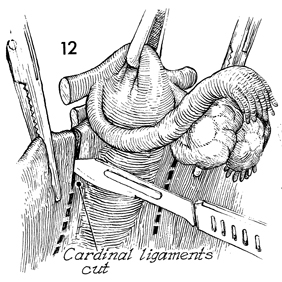
Cephalad retraction is placed
on the dome of the cervical stump. Straight Ochsner clamps are
applied to the lateral edge of the cervix and allowed to slide
off into a "groove" immediately lateral to the cervix, clamping
any remaining portions of the uterine vessels and the cardinal
ligament. The cardinal ligament is then transected with a scalpel,
leaving an adequate stump protruding from the Ochsner clamp to
prevent retraction of the stump of the cardinal ligament through
the clamp. |
A second or, possibly third application of
the Ochsner clamp is needed to completely clamp and transect
the cardinal ligament. The last application of the Ochsner clamp
encompasses in one bite the remaining portion of the cardinal
ligament and the uretrosacral ligament. By uniting the cardinal
and uretrosacral ligaments in one pedicle, the first step in
resuspension of the vaginal cuff is created. This is incorporated
into the angle of the vagina in later steps to facilitate suspension
and to prevent enterocele. |
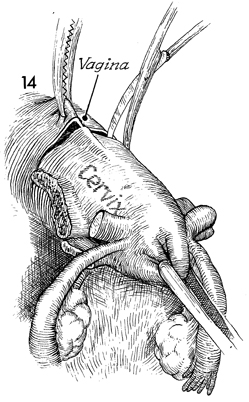
With cephalad retraction on the cervical
stump, the anterior wall of the vagina is picked up by an Ochsner
clamp, and the vagina is entered with curved Mayo scissors or
by a stab wound with a scalpel. The curved Mayo scissors is then
used to transect the remaining vaginal canal, and the cervical
stump, the tubes, and the ovaries are removed. |
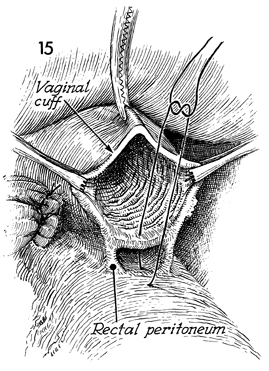
The space between the rectum and the vagina
is closed with 0 synthetic absorbable suture. |
The 0 synthetic
absorbable suture is continued in a running lock fashion around
the edge of the vagina. Care is taken to place several sutures
into the stump of the uretrosacral and cardinal ligaments to
firmly attach them to the angle of the vagina. |
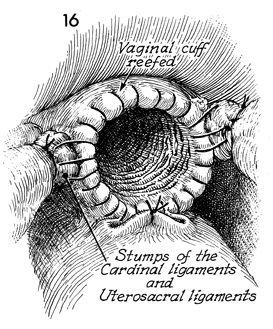
The peritoneum of the pelvis is reestablished
with a running 3-0 synthetic absorbable suture approximately
the anterior peritoneum to the posterior peritoneum. |
|
|
