|
||||||||
Directed Biopsy of the Cervix at Colposcopy Endocervical
Curettage Conization
of the Abdominal
Excision Correction
of an Incompetent Cervix Correction
of an Incompetent Cervix |
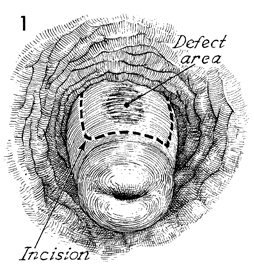
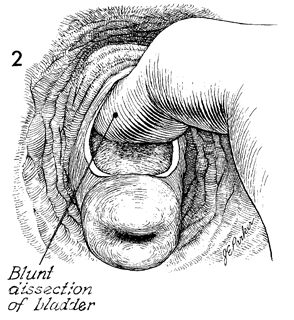
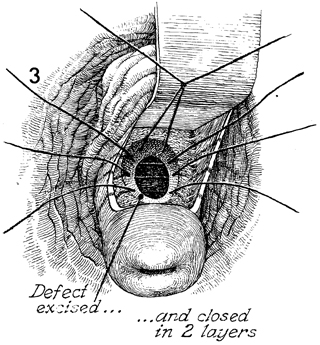
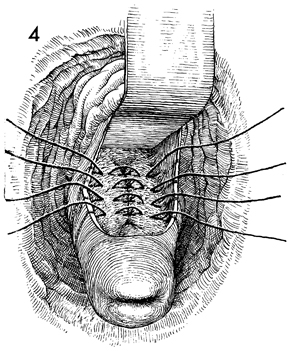
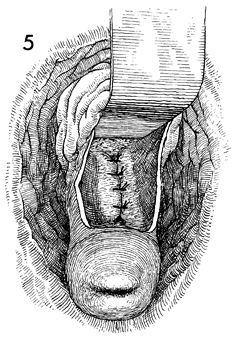
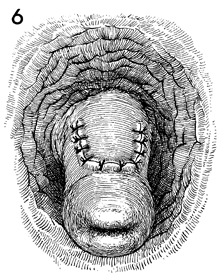
Correction of an Incompetent Cervix by the Lash Operation Patients with habitual second-trimester abortions occasionally show a defect in the wall of the cervix. This is usually at the 12 o'clock position at the internal cervical os and may be related to failure of fusion of the Mullerian duct. In any case, it results in a weakened internal cervical os. Repair is best performed in the nonpregnant state. The purpose of the Lash operation is to correct the defect in the cervical wall and restore competence to the cervix, thereby allowing gestation to proceed to term. Physiologic Changes. The cervix regains the strength to hold the developing fetus in utero until term, thus preventing second-trimester abortion. Points of Caution. Patients undergoing the Lash operation
should be delivered at term by cesarean section. Dilation and effacement
of the cervix following this procedure are unpredictable. Care must be taken to ensure that the bladder is properly retracted in order to prevent the placement of sutures through the bladder in the closing of the cervical defect. Technique
|
|||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.