
Cervix
Biopsy
of the Cervix
Directed
Biopsy of the Cervix at Colposcopy
Endocervical
Curettage
at Colposcopy
Conization
of the
Cervix by the Loop Electrical Excision Procedure (LEEP)
Cryosurgery of Cervix
Conization of Cervix
Abdominal
Excision
of the Cervix Stump
Correction
of an Incompetent Cervix
by the Shirodkar
Technique
Correction
of an Incompetent Cervix
by the McDonald
Operation
Correction
of an Incompetent Cervix
by the Lash Operation |
Correction of an Incompetent Cervix by the Shirodkar Technique
Patients who have habitually experienced second-trimester
abortions may have an incompetent cervical os. Of the several surgical
alternatives available to correct this problem, the Shirodkar technique,
with fascia lata used, is an excellent choice for patients in the nonpregnant
state.
The purpose of the operation is to restore competence
to the cervix and thereby prevent the cervix from dilation during the
second-trimester pregnancy.
Physiologic Changes. The restoration of appropriate
strength to the internal cervical os prevents sudden dilation as the
pregnancy progresses.
Points of Caution. Patients having this operation
should be delivered at term by cesarean section.
Care must be taken to adequately mobilize the bladder to prevent injury
from application of the fascia strap.
If the tunnel made on the lateral side of the cervix is made too high,
the uterine vessels may be perforated, and copious hemorrhage may result.
Technique
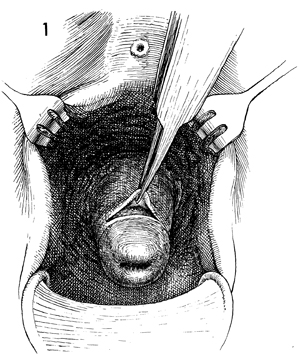
The patient is placed in the dorsal lithotomy
position. The vulva and vagina are prepped with a surgical soap
solution. A weighted posterior retractor is placed in the vagina,
and the cervix is grasped with a wide-mouthed tenaculum on the
anterior lip. A transverse incision approximately 2-3 cm wide
is made at the junction of the vaginal mucosa and the portio
of the cervix. The incised edge of the vagina is picked up with
an Allis clamp or thumb forceps. |
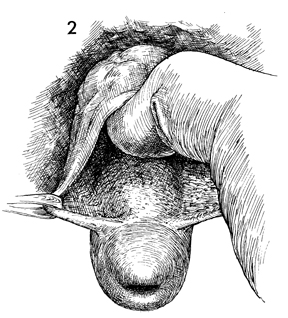
Allis clamps are applied to the lateral edge
of the transverse incision, and a gloved finger is used to dissect
the bladder off the cervix. The bladder should be dissected up
to the vesicouterine peritoneal fold, thus avoiding injury when
the strap is placed. |
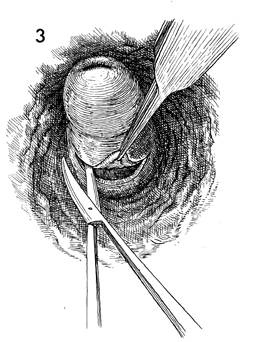
The posterior vaginal epithelium overlying
the cul-de-sac is exposed. A transverse incision is made approximately
2-3 cm at the junction of the posterior vaginal mucosa and the
cervical portio. With Metzenbaum scissors, the peritoneum of
the cul-de-sac is dissected from the posterior cervix. |
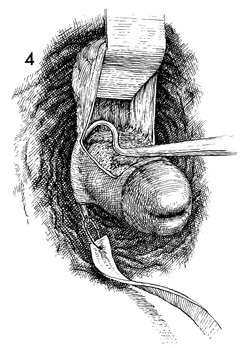
A piece of fascia lata that has been previously
taken from the lateral thigh (see Vagina and Urethra, for the
Goebell-Stoeckel fascia lata sling procedure including the technique
for obtaining the strip of fascia lata) is used for the Shirodkar
strap. An aneurysm needle is maneuvered under the vaginal mucosa
from the anterior incision into the posterior incision. A suture
of 2-0 Prolene is placed in the end of the fascia lata strap
and tied to the aneurysm needle. |
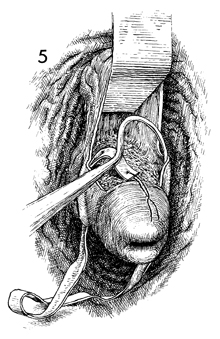
The fascia strap is pulled from the posterior
transverse incision into the anterior transverse incision. In
a similar manner, the other aneurysm needle is used to dissect
under the left side of the remaining vaginal mucosa and likewise
is attached to the opposite end of the fascia strip with 2-0
Prolene. |
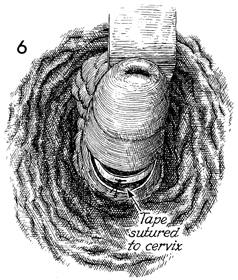
The fascia lata strap is
fixed to the posterior surface of the cervix with a single interrupted
2-0 synthetic absorbable suture. |
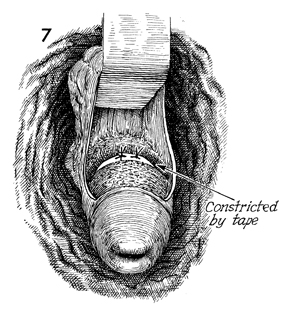
A right-angle retractor lifts the bladder
up and away from the anterior cervix; the fascia lata strap is
trimmed to fit snugly around the cervix at the level of the internal
os. The fascia strap is anchored to the anterior cervical tissue
with several interrupted 2-0 Prolene sutures. |
The anterior vaginal mucosa
is returned to position and resutured with interrupted 3-0 synthetic
absorbable suture. |
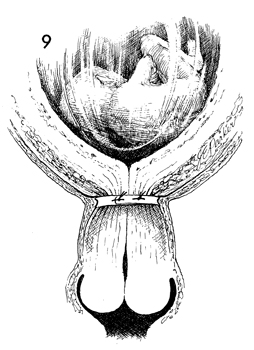
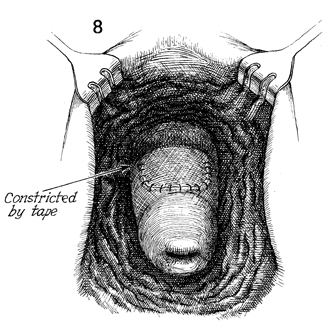
This illustrates the results of the operation
in the midplane. The internal os is closed enough to admit only
a uterine sound or a 4-mm Hegar dilator. Thus, it becomes obvious
that cesarean section will have to be performed to accommodate
delivery. |
|
|
