
Uterus
Dilatation
and Curettage
Suction
Curettage
for Abortion
Management
of Major
Uterine Perforations
From Suction Curet or
Radium Tandem
Cesarean
Section
Myomectomy
Jones
Operation
for Correction of
Double Uterus
Hysteroscopic
Septal
Resection by Loop
Electrical Excision
Procedure (LEEP) for
Correction of a Double
Uterus
Manchester
Operation
Richardson Composite Operation
Total
Vaginal Hysterectomy
Total
Abdominal
Hysterectomy With
and Without Bilateral
Salpingo-oophorectomy
Laparoscopy-Assisted Vaginal
Hysterectomy |
Dilatation and Curettage
Dilatation and curettage unrelated to pregnancy is best performed
with the patient under general anesthesia to allow the gynecologist
to perform a more thorough pelvic examination.
The purpose of the operation
is to remove as much hyperplastic, proliferative, and necrotic endometrium
as possible to allow an accurate pathologic diagnosis to be made and
to arrest dysfunctional uterine bleeding. Excessive bleeding will usually
discontinue for at least several months.
Physiologic Changes. Removal of the endometrium back
to the stratum basale will not change the physiology of the hypothalamic-pituitary-ovarian
axis in regard to ovulation.
Points of Caution. Care must be taken in dilating
the cervix to avoid peroration of the uterus.
Technique
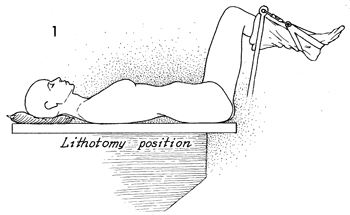
The patient is placed in the dorsal lithotomy
position with the legs in appropriate gynecologic stirrups. |

A thorough bimanual examination, including
a rectovaginal examination, should be performed prior to the
procedure.
The perineum and vagina should
be washed with surgical soap. Shaving the perineal hair, however,
is not necessary for this procedure. |
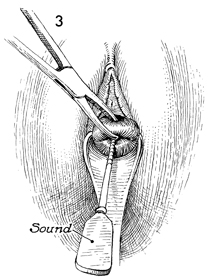
Adequate exposure to the cervix can be achieved
by the use of a Sims retractor. Some gynecologists prefer a weighted
posterior retractor, but in most cases this is unnecessary. The
procedure is begun by grasping the anterior lip of the cervix
with a wide-mouthed Jacobs tenaculum. The endometrial cavity
is sounded for both depth and direction. |
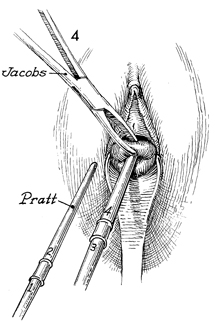
The cervical canal is progressively
dilated with Pratt dilators until a diameter of approximately
8 mm is reached. |
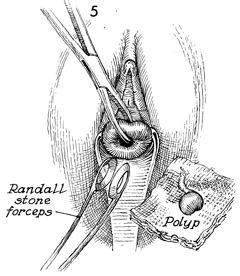
A ureteral stone forceps is helpful in exploring
the uterine cavity and searching for polyps. Polyps can frequently
be missed by the sharp curet itself. If polyps are found, they
should be removed by twisting them from their stalks. They should
be sent to the pathology laboratory in a separate specimen. |
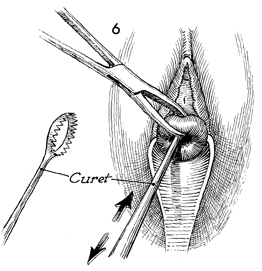
A sharp curet
is advanced through the dilated cervical canal to the fundus.
The endometrial cavity is curetted with a systematic back-and-forth
movement of the curet so that all possible endometrium is sampled. |
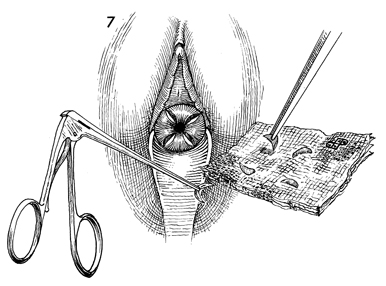
The cervix should be stained
with Lugol's solution, and four random quadrant biopsies should
be taken from the squamocolumnar junction. |
|
|
