
Uterus
Dilatation
and Curettage
Suction
Curettage
for Abortion
Management
of Major
Uterine Perforations
From Suction Curet or
Radium Tandem
Cesarean
Section
Myomectomy
Jones
Operation
for Correction of
Double Uterus
Hysteroscopic
Septal
Resection by Loop
Electrical Excision
Procedure (LEEP) for
Correction of a Double
Uterus
Manchester
Operation
Richardson Composite Operation
Total
Vaginal Hysterectomy
Total
Abdominal
Hysterectomy With
and Without Bilateral
Salpingo-oophorectomy
Laparoscopy-Assisted
Vaginal Hysterectomy |
Suction Curettage for Abortion
Suction curettage has proven to be the most efficacious technique
for evacuation of the uterus in the first trimester of pregnancy. It
has advantages over sharp curettage in that it has a lower incidence
of uterine perforation and less blood.
The purpose of the operation is to evacuate the gravid
uterus in the first trimester.
Physiologic Changes. The use of a
strong vacuum through a suction catheter placed through the dilated
cervix into the uterine cavity rapidly shears away the first-trimester
placenta from the uterine wall.
When a vacuum pump producing 70 mm Hg
and 100 mL of airflow per minute is used, the products of conception
are rapidly separated from the uterine wall, allowing their removal
from the endometrial cavity and inducing uterine contraction, thereby
reducing blood loss.
Points of Caution. Care must be taken
to determine the length of gestation of the pregnancy. This should
be done by history and by physical examination of the pelvis. In addition,
the uterine cavity should be accurately measured with a sound prior
to initiating the procedure. In this way, pregnancies exceeding 13
weeks should be diagnosed, and suction abortion performed, in those
circumstances where the potential benefits outweigh the risks of performing
a second-trimester abortion with the suction technique.
The surgeon
should be sure that adequate airflow through the suction pump is maintained
at all times. An airflow in the system of approximately 100 mL/minute
is preferred. For most standard suction curettage machines, this means
turning the pump to the maximum setting. Reduced or low airflow through
the system allows retained products of conception and therefore increases
the risk of hemorrhage and postpartum infection.
If
perforation of the uterus is suspected, the vacuum should be turned
off, and the curet should be removed with caution to prevent injury
to the intestine.
Technique
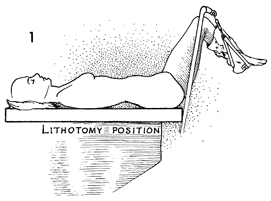
The patient is placed in the dorsal lithotomy
position after appropriate anesthesia (general, regional, or
local) has been administered. |
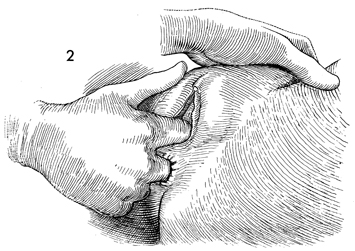
A careful pelvic examination is performed
to accurately ascertain the gestational size of the uterus. |
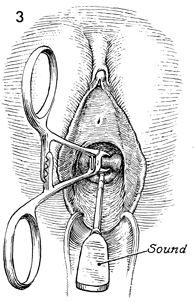
A Sims posterior retractor is used to obtain
adequate exposure to the upper vagina and cervix. Lateral retractors
or self-retaining retractors are rarely needed for this procedure.
The anterior lip of the cervix is grasped
with a wide-mouthed Jacobs tenaculum. Single-toothed tenacula
should be avoided, as they tend to tear the pregnant cervix.
A uterine sound is passed through the undilated cervix until
the fundus is reached. The length of the uterine cavity is recorded. |
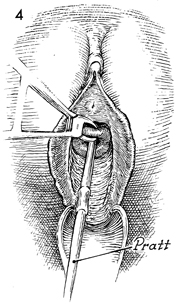
Tapered cervical dilators,
such as Pratt dilators, are used to progressively dilate the
cervix, usually to 10 mm in diameter. Nontapered dilators, such
as Hegar dilators, should be avoided because they are difficult
to pass through the cervix, particularly in nulliparous patients,
and produce a greater amount of cervical trauma. |
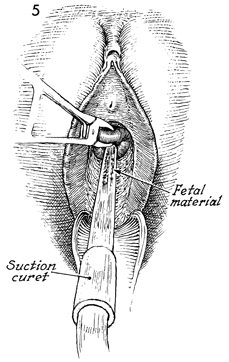
After appropriate dilatation, a suction
cannula is introduced through the cervix. We prefer large-diameter
straight suction cannulae, such as 10-mm straight cannulae, rather
then the curved or angulated variety. This is because 360° arcs
of the cannulae must be made to adequately remove all gestational
tissue. When 360° arcs are made with angulated cannulae,
the diameter of the arc created in the intrauterine cavity by the
angulated suction cannulae is excessive.
The suction curet should be
introduced all the way to the fundus. |
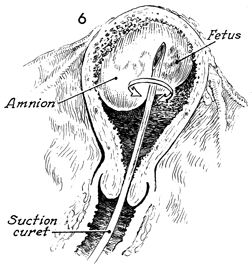
The suction is applied to
the curet. The curet is rotated in a 360° arc and is slowly
withdrawn in 1-cm increments.
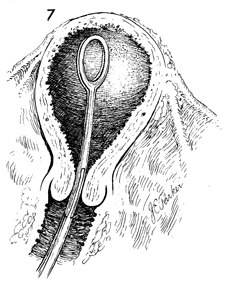
The suction
curet should be introduced 2-3 times to ensure that all products
of conception have been adequately removed.
It is efficacious
at this point to administer 50 international units of Pitocin
in an intravenous drip and 0.2 mg of Methergine given intravenously.
This has significantly reduced blood loss by inducing uterine
contraction. |
An ovum or sponge forceps is
introduced into the endometrial cavity and are opened, closed,
and withdrawn several times to ensure that all gestation tissue
has been removed.
The patient is observed for
2 hours for hemorrhage prior to discharge. |
|
|
