|
||||||||||||||||||||
Suction
Curettage Management
of Major Jones
Operation Richardson Composite Operation Total
Abdominal |
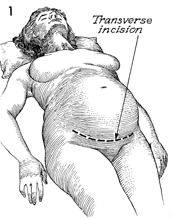
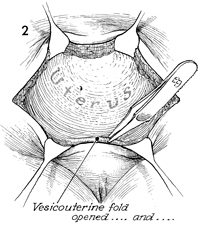
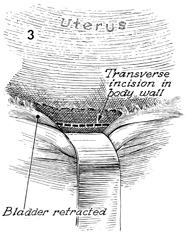
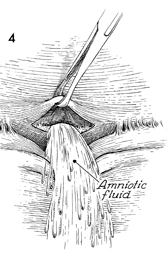
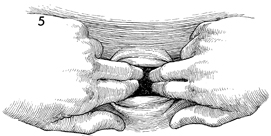
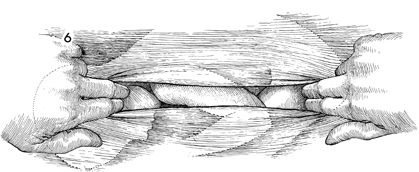
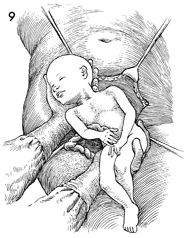
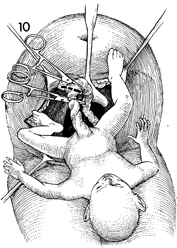
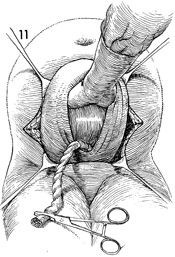
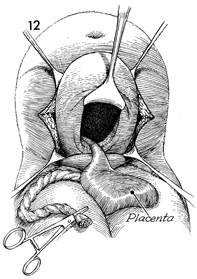
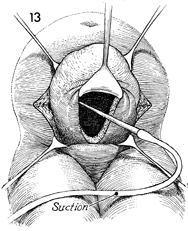
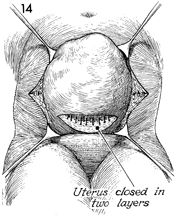
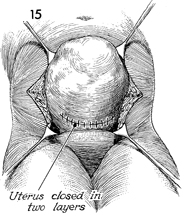
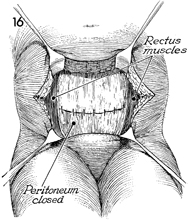
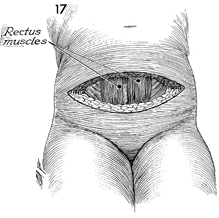
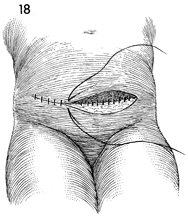
Cesarean Section Cesarean section, a life-saving operation for both fetus and mother, accounts for approximately 20% of deliveries in the United States today. The lower cervical transverse incision for this operation has become the accepted technique, except in cases in which compound presentations require the classic vertical incision in the fundus of the uterus. The purpose of the operation is to deliver the fetus through the abdomen in instances where vaginal delivery would be either impossible or dangerous to the life or health of the mother and/or fetus. Physiologic Changes. There are many differences in the physiologic changes between vaginal delivery and cesarean section. Fetuses delivered by ceaseran section may have a higher incidence of respiratory distress syndrome. On the other hand, vaginal delivery with dystocia can produce central nervous system damage. Further discussion involving the physiology of cesarean section is beyond the scope of this text, and the reader is referred to the obstetrical literature for additional information. Points of Caution. The anesthesia for cesarean section should be selected with care. An epidural regional block is recommended, since this has the least chance of causing fetal depression. If general anesthesia is to be used, the anesthesiologist should be consulted to ensure proper timing between the infusion of the rapid-acting barbiturates and delivery of the baby in order to minimize any depressing effect on the central nervous system of the fetus. Care should be exercised in dissecting the bladder off the lower uterine segment to prevent laceration of the bladder during the procedure. If, by chance, excessive manual stretching of the transverse incision should lacerate the uterine vessels in the broad ligament, this ligament should be opened. The uterine vessels should then be carefully dissected out and individually ligated to prevent postoperative hematoma and possible damage to the underlying ureter. Technique
|
|||||||||||||||||||



Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.