|
||||
Bartholin's Gland Cyst Marsupialization Excision of Vulvar Skin, with Split-Thickness Skin Graft Vaginal
Outlet Closure of Wide Local Excision of the Vulva Wide
Local Excision Alcohol
Injection Cortisone
Injection Excision
of the |
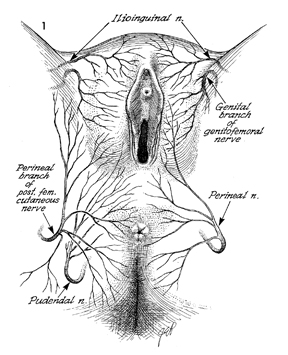
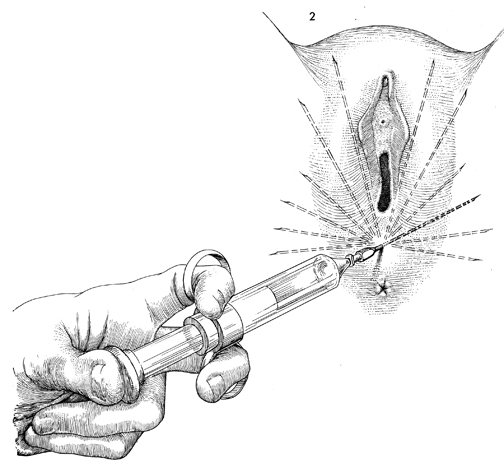
Cortisone Injection of the Vulva In patients with chronic pruritus of the vulva, subcutaneous injection of the vulva with a fluorinated cortisone preparation will often relieve the patient and break the vicious cycle of itching, scratching, excoriation, and irritation of cutaneous nerves. Pruritus of the vulva is often associated with parakeratosis that does not allow steroid cream to penetrate the skin and reach the important subdermal area. The injection must cover the entire vulva. Particular attention must be given to those areas that the patient designates as especially troublesome. Physiologic Changes. Pruritus of the vulva is eliminated. Cortisone reduces the inflammatory reaction and improves the vascular supply and thus improves the nutrition of the vulvar skin. Points of Caution. Care must be exercised to inject the entire vulva and to avoid penetration of the perineal branches of the pudendal artery and vein. Technique With the patient under general or local anesthesia in the lithotomy position, the surgeon outlines the inflamed areas of the vulva.
|
|||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.