|
||||||||
Bartholin's Gland Cyst Marsupialization Excision of Vulvar Skin, with Split-Thickness Skin Graft Vaginal
Outlet Closure of Wide Local Excision of the Vulva Wide
Local Excision Alcohol
Injection Cortisone
Injection Excision
of the |
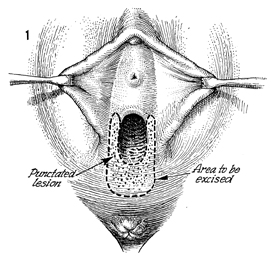
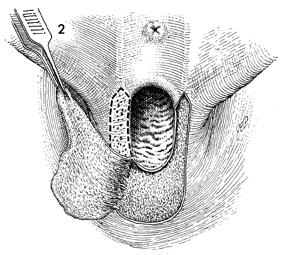
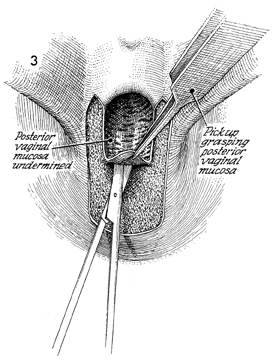
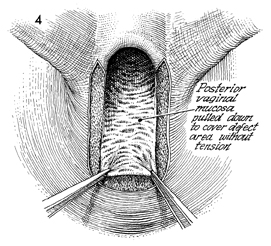
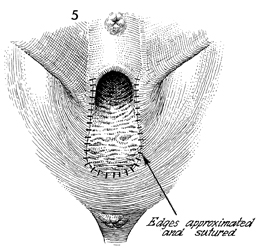
Excision of Vestibular Adenitis Nonspecific inflammation in the glands in the vestibule of the vulva, termed vulvodynia by the International Society for the Study of Vulva Disease, has been broken down into three categories: (1) vestibulitis, (2) squamous papillomatosis (vulvar dermatoses, cyclic candidiasis, squamous papillomatosis), and (3) essential vulvodynia. All too often these patients have a 6-month or greater history of being treated with anti-inflammatory, antifungal, and antibacterial agents prescribed by numerous physicians. All to often these patients undergo laser vaporization that results in more constriction and dyspareunia to the vaginal outlet. Excision of the hymen along with the adjacent inflamed glands has produced relief of symptoms in about 75-90% of cases. Where there is diagnostic uncertainty, every effort should be made to treat these patients with conservative therapy prior to surgical resection. Once surgical resection has been chosen, it is important that the entire vestibular glandular area involved in the process be surgically removed. Physiologic Changes. The predominate physiologic change in resection of vestibular adenitis is removal of the inflamed vestibular glands that cause severe pain and dyspareunia. The absence of this tissue produces little change in the physiology of the functioning vagina and vulva. Points of Caution. The involved area of the vestibule should be carefully marked out under superior light and, if possible, with optical magnification to ensure that an adequate excision of the vestibular adenitis is made. Thorough mobilization and advancement of the posterior and lateral vaginal wall sufficient to come out on the posterior fourchette without tension should be performed. If the posterior vaginal wall is brought out under tension, it will retract, and contracture of the vaginal outlet with its sequela will occur. Technique
|
|||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.