|
||||||||||
Bartholin's Gland Cyst Marsupialization Excision of Vulvar Skin, with Split-Thickness Skin Graft Vaginal
Outlet Closure of Wide Local Excision of the Vulva Wide
Local Excision Alcohol
Injection Cortisone
Injection Excision
of the |
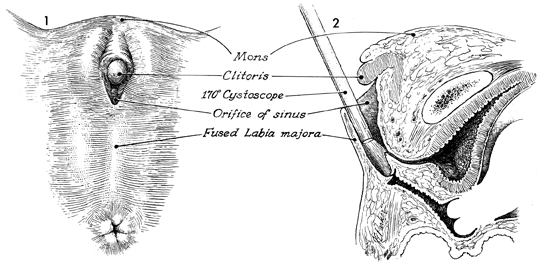
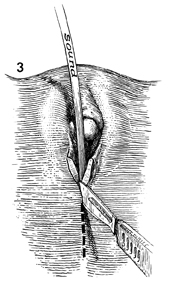
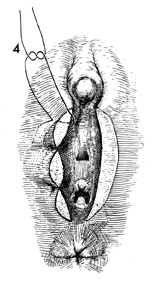
Release of Labia Fusion Labial fusion is secondary to a urogenital sinus deformity, and in the majority of cases the labia separate on their own or with applications of estrogen cream. There are, however, some cases where the fusion is not amenable to conservative management and surgical intervention is required. The importance of preoperative evaluation prior to surgical management is vital to the success of the procedure. The gender of some patients may be unclear. The clitoris is mistaken for a micropenis, and the fused folds of the labia may be mistaken for a scrotum with undescended testes. Appropriate cytogenetic studies are indicated. An examination under anesthesia with careful probing of all openings under the clitoris/penis should be performed. Only after the patient has been adequately evaluated should surgical management be started. Physiologic Changes. The fused labia are opened, resulting in a normal vaginal canal. Points of Caution. Care should be taken to identify all genital canals within the pelvis. A silver wire probe and uterine sound should be gently inserted into the various canals under general anesthesia in order to identify each opening prior to making an incision into the labia. Technique
|
|||||||||


Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.