|
||||||
Bartholin's Gland Cyst Marsupialization Excision of Vulvar Skin, with Split-Thickness Skin Graft Vaginal
Outlet Closure of Wide Local Excision of the Vulva Wide
Local Excision Alcohol
Injection Cortisone
Injection Excision
of the |
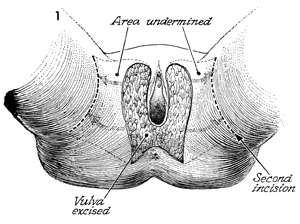
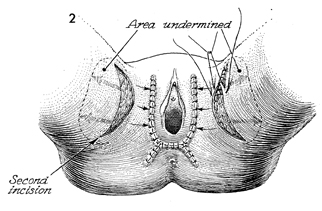
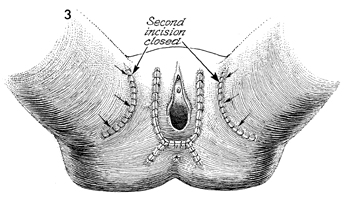
Closure of Wide Local Excision Early intraepithelial neoplasias of the vulva frequently have multicentric foci of disease. To adequately excise these lesions with an appropriate surgical margin of 2 cm, wide local excision of the vulva may be required. This kind of excision can be closed by mobilizing the skin lateral to the incision and creating a relaxing incision at an appropriate place to allow coverage of the vulvar defect. This technique provides a skin flap with the blood supply coming from both the mons pubis femoral area and the skin covering the buttocks. Physiologic Changes. The neoplastic lesion is excised, and primary closure of the wound is made without distortion of the vulva or stricture of the vaginal orifice. Points of Caution. Prior to excision of the lesion, the margin of normal skin to be removed is measured with a centimeter ruler and outlined with a marking pen. This will ensure adequate margins around the neoplastic lesion. The skin flap must be adequately
mobilized in order to move it easily. Hemostasis is essential. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.