
Vulva
and Introitus
Biopsy
of the Vulva
Excision
of Urethral Caruncle
Bartholin's
Gland Cyst Marsupialization
Excision
of Vulvar Skin, with Split-Thickness Skin Graft
Bartholin's
Gland Excision
Vaginal
Outlet
Stenosis Repair
Closure
of Wide Local Excision of the Vulva
Wide
Local Excision
of the Vulva, With Primary Closure or Z-plasty Flap
Alcohol
Injection
of the Vulva
Cortisone
Injection
of the Vulva
Merring Operation
Simple
Vulvectomy
Excision
of the
Vulva by the Loop Electrical Excision Procedure (LEEP)
Excision
of
Vestibular Adenitis
Release
of Labial Fusion
Hymenectomy
Excision Of Hypertrophied Clitoris
|
Biopsy
of the Vulva
Gross lesions of the vulva often seem to be benign.
However, a gross lesion of any description on the external or internal
female genitals is suspicious, and with rare exceptions, a biopsy should
be taken for histologic analysis.
A histologic specimen encompassing pathologic as well
as normal squamous epithelium is obtained from the vulva.
Physiologic Changes: None
Point of Caution: The biopsy should
provide reliable pathologic specimens; tangential cutting may lead
to misinterpretation.
Technique
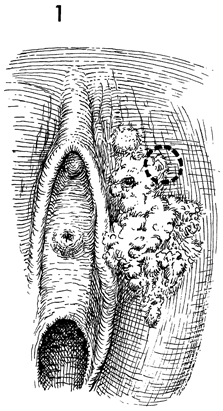
The patient is placed in the dorsal
lithotomy position. The area of pathologic abnormality is cleansed
with antiseptic solution, and the proposed biopsy site is selected. |
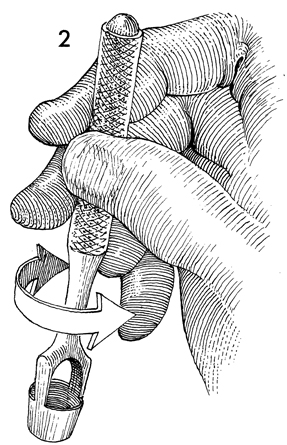
A Keys punch, commonly used by dermatologists,
is excellent for this purpose. The 5-7 mm size allows appropriate
pathologic specimens to be taken without leaving a defect large
enough to require sutures. |

The area is anesthetized with
1 mL of 1% Xylocaine injected subcutaneously. The biopsy is then
taken by rotating the Keys punch over the skin in 180° arches.
|
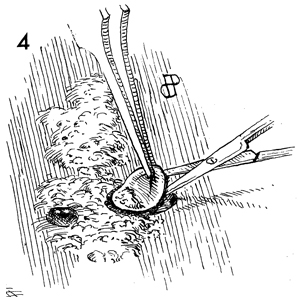
A delicate forceps
is used to elevate one margin of the biopsy, and a small cuticle
scissors is used to dissect the biopsy off its bed. A suture
is rarely required, and no dressing is applied. |
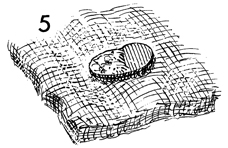
The biopsy is oriented on a piece of saline-soaked
gauze, enabling the pathologist to perform ideal sections.
|
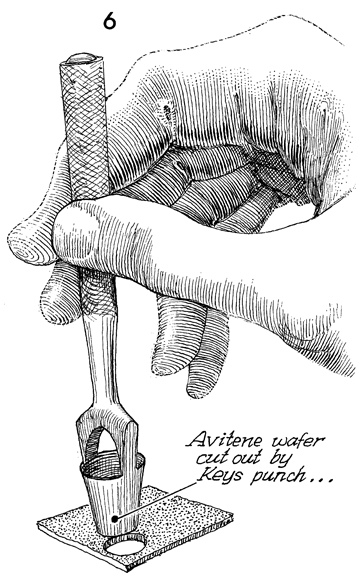
If necessary, a plug can
be cut from an Avitene or Gelfoam wafer by using the sharp edge
of the Keys punch. |
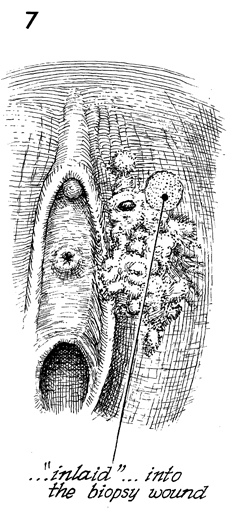
This plug can be placed in
the biopsy defect to provide hemostasis. It will act as an
excellent dressing for the wound and, in most cases, omit the
need for suturing. The patient is instructed to keep the site
clean with ordinary soap and water and to wear a perineal pad
as required.
|
|
|
