|
||||||||
Bartholin's Gland Cyst Marsupialization Excision of Vulvar Skin, with Split-Thickness Skin Graft Vaginal
Outlet Closure of Wide Local Excision of the Vulva Wide
Local Excision Alcohol
Injection Cortisone
Injection Excision
of the |
Excision
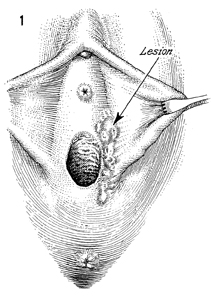
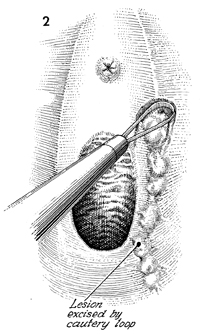
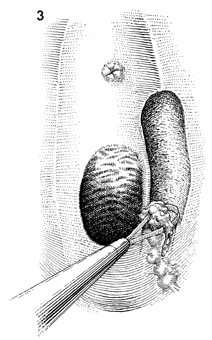
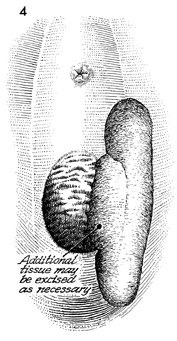
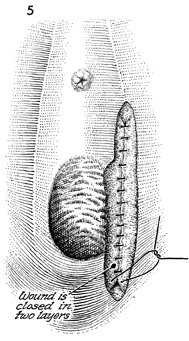
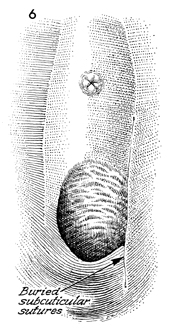
of the Vulva by the Loop The technique for removal of small lesions from the vulva, e.g., condyloma acuminatum and in situ carcinomas, has varied over time with the technologic facilities available to the surgeon. The techniques have ranged from sharp knife, to laser vaporization, to the currently popular electrosurgical excision. Electrosurgical excision has the advantage of being inexpensive and available as an office or outpatient clinic procedure. Local anesthesia is adequate and should be performed 5-6 minutes prior to the excision. Smoke evacuation is important for two reasons: (1) The human papilloma virus (HPV) has been shown to survive flumen of the electrosurgical and laser procedure; and (2) smoke seen arising from the vulva might incite anxiety and reduce the patient's ability to cooperate. With the advent of laser vaporization, many of these excised lesions of the vulva were left open to epithelialize over 4-6 weeks by second intention. We always close laser vaporization and electrosurgical wounds. Physiologic Changes. The excision of in situ carcinoma reduces the breakdown and excoriation of the vulva, with constant drainage of these lesions. Untreated condylomata can break down, become infected, and cause undesirable drainage from the vulva. Points of Caution. The electrosurgical instrument should be set on a blend between the cutting and coagulation current. The predominate wattage should be used for cutting, and the smaller wattage should be devoted to coagulation in order to reduce thermal injury to the tissue. For most standard electrosurgical machines, we prefer a wattage of 60 for cutting to 10-20 for coagulation. Small areas of bleeding can be lightly touched with the ball cautery on coagulation. Technique
|
|||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.