
Vulva
and Introitus
Biopsy
of the Vulva
Excision
of Urethral Caruncle
Bartholin's
Gland Cyst Marsupialization
Excision
of Vulvar Skin, with Split-Thickness Skin Graft
Bartholin's
Gland Excision
Vaginal
Outlet
Stenosis Repair
Closure
of Wide Local Excision of the Vulva
Wide
Local Excision
of the Vulva, With Primary Closure or Z-plasty Flap
Alcohol
Injection
of the Vulva
Cortisone
Injection
of the Vulva
Merring Operation
Simple
Vulvectomy
Excision
of the
Vulva by the Loop Electrical Excision Procedure (LEEP)
Excision
of
Vestibular Adenitis
Release
of Labial Fusion
Hymenectomy
Excision Of Hypertrophied Clitoris |
Bartholin's
Gland Excision
Excision of the Bartholin's gland has been called the
"bloodiest little operation in gynecology." It is indicated for persistent
and recurrent Bartholin's gland abscess and cyst. The key to successful
excision is hemostatic control of the copious blood supply to the gland.
The purpose of the operation is to remove the entire
Bartholin's gland.
Physiologic Changes. Bilateral removal
of Bartholin's gland eliminates the secretion of fluid from the gland
that is useful as a vaginal lubricant. In the well-estrogenized vagina,
however, this is generally not a clinical problem.
Points of Caution. Meticulous hemostasis
is essential. The branches of the pudendal artery are frequently lacerated
during excision of the Bartholin's gland. They must be carefully identified,
clamped, and tied, or postoperative vulvar hematoma will result.
Technique
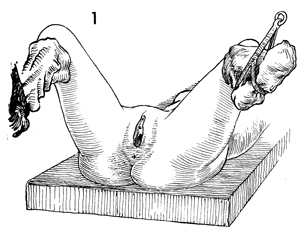
The patient is placed in the dorsal lithotomy
position, and the perineum is prepped and draped. |
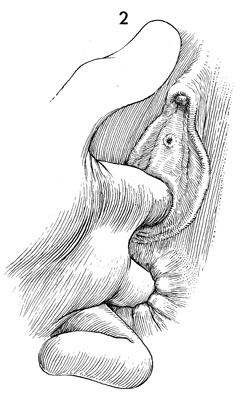
Careful rectovaginal examination
is performed to outline the entire Bartholin's gland cyst or abscess. |
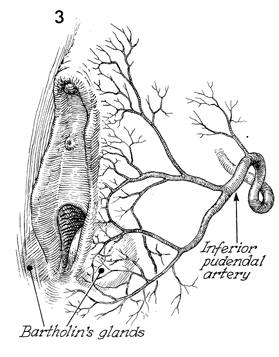
To control bleeding, it is
essential that the surgeon understand the vascular supply to
the labia and vagina.
|
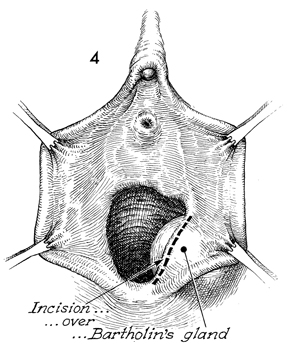
The labia are retracted laterally
with several Allis clamps. For resection of the Bartholin's gland,
it is preferable to make the incision over the vaginal mucosa,
directly over the meatus of the gland, rather than over the labia
majora. Healing in this area appears to be faster and less painful
for the patient than does healing to an incision in the skin of
the labia. |
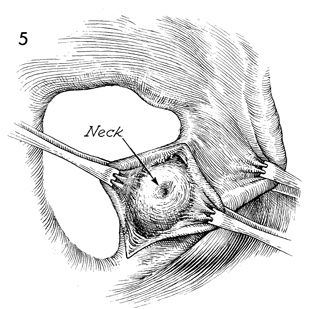
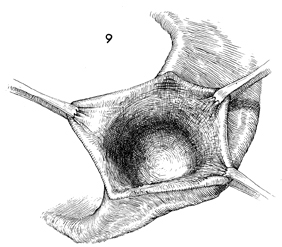
The vaginal mucosa is retracted medially, and the
skin of the introitus is retracted laterally to expose the wall
of the gland. Its meatus may be seen if not distorted by old infection
and scarring. |
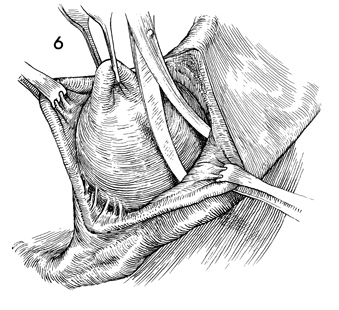
A small Metzenbaum scissors is used to lyse the
filmy adhesions between the wall of the abscess or cyst and the
overlying vaginal mucosa and subcutaneous tissue of the labia
majora. Either forceps or an Allis clamp is placed on the wall
of the cyst. The wall is retracted to allow adequate dissection
and identification of the blood supply to the gland from branches
of the pudendal artery.
|
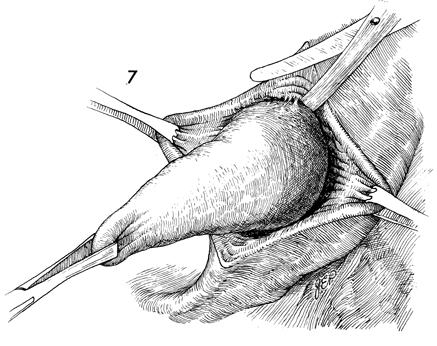
It is important to excise the entire gland.
Incomplete removal may lead to a recurrence of the cyst or abscess. |
The last few filmy adhesions to the gland
are incised with Metzenbaum scissors, and the gland is removed. |
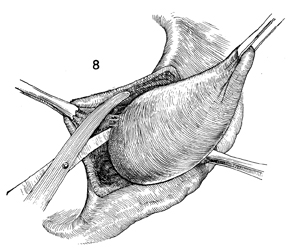
After removal of the gland, there is frequently
bleeding from the wound. |
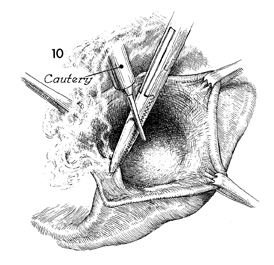
Care must be taken that meticulous
hemostasis is carried out throughout the bed of the gland. Hemostasis
frequently requires electrocoagulation and suture ligation. |
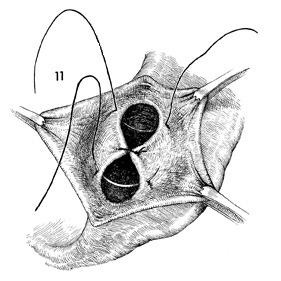
The bed of the gland should be closed with
interrupted 3-0 absorbable suture to eliminate dead space. |
A small closed suction drain is inserted
into the wound and sutured into place with interrupted 5-0 absorbable
suture. This prevents the drain from being prematurely dislodged
but allows for easy removal. |
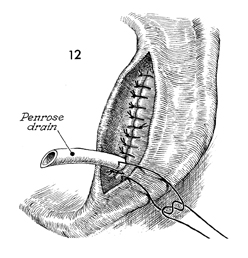
The closure of the vaginal mucosa to the
skin of the introitus is completed with interrupted 3-0 Dexon
suture.
The closed suction drain is removed
on the third or fourth day when there is no further drainage.
Cultures
of the abscess should be made. Frequently, gonococci, streptococci,
or other organisms are found; therefore, preoperative antibiotics
are used in most cases.
On the third postoperative day,
the patient is placed on a regimen of hot sitz baths and is given
a stool softener and laxative.
Sexual intercourse can usually be
resumed in 4 weeks.
|
|
|
