
Vagina
and Urethra
Anterior Repair and Kelly
Plication
Site Specific Posterior Repair
Sacrospinous
Ligament Suspension of the Vagina
Vaginal Repair of Enterocele
Vaginal Evisceration
Excision of
Transverse Vaginal Septum
Correction of
Double-Barreled Vagina
Incision
and Drainage of Pelvic Abscess via the Vaginal Route
Sacral Colpoplexy
Le Fort Operation
Vesicovaginal Fistula
Repair
Transposition
of Island Skin Flap for Repair of Vesicovaginal Fistula
McIndoe Vaginoplasty
for Neovagina
Rectovaginal Fistula
Repair
Reconstruction of
the Urethra
Marsupialization
of a Suburethral Diverticulum by the Spence Operation
Suburethral
Diverticulum via the Double-Breasted Closure Technique
Urethrovaginal
Fistula Repair via the Double-Breasted Closure Technique
Goebell-Stoeckel
Fascia Lata Sling Operation for Urinary Incontinence
Transection
of Goebell-Stoeckel Fascia Strap
Rectovaginal
Fistula Repair via Musset-Poitout-Noble Perineotomy
Sigmoid
Neovagina
Watkins Interposition Operation |
Vaginal Evisceration
Although vaginal evisceration of the intestine is rare and usually
follows hysterectomy within the immediate postoperative period, some
cases have been reported years after surgery. The problem can arise
after abdominal as well as vaginal hysterectomy and also as a sequela
of the rupture of large enteroceles, with or without previous hysterectomy.
A contemporary source of vaginal evisceration has been suction curettage
for termination of pregnancy. During this procedure, if the uterine
wall is perforated, the small intestine can be sucked into the eye
of the vacuum curet and pulled through the perforation in the uterus
and out into the vagina.
The etiology of vaginal evisceration, except for that associated with
suction for termination of pregnancy, is not associated with any specific
pattern of events.
Physiologic Changes. The anatomy of the small bowel
and the length of its mesentery make vaginal evisceration difficult.
If a laceration occurs in the mesentery of the small bowel, evisceration
is more likely. All patients with vaginal evisceration must undergo
an exploratory laparotomy with extensive inspection of the small bowel
and its mesentery. Because of the unique blood supply to the small
bowel, an undiagnosed laceration in its mesentery may result in necrosis.
This may explain why the overall mortality from vaginal evisceration
is as high as approximately 10%.
Points of Caution. No attempt should be made to simply
replace the bowel through the vaginal cuff and close it. All patients
should be treated with an abdominoperineal approach. The entire length
of the small bowel should be carefully inspected for areas of devascularization.
A classic repair for obliteration of the cul-de-sac
through use of the vaginal cuff, the uterosacral ligaments, and the
anterior rectal wall should be made to reduce the chance of recurrence.
Technique
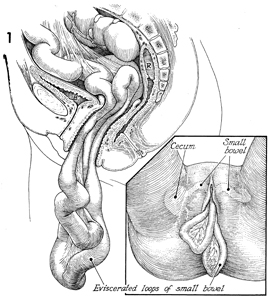
A sagittal view of the evisceration is
shown. In this particular case, the evisceration has occurred
through an open vaginal cuff after a hysterectomy. B identifies
the bladder; and R, the rectum. The insert to
Figure 1 shows the perineal view with the anatomical location
of the cecum and other loops of small bowel.
|
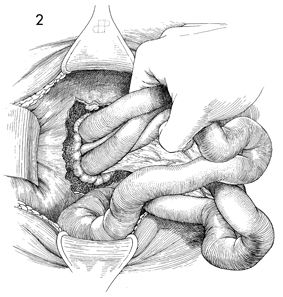
An exploratory laparotomy has
been performed, and the loops of the eviscerated small bowel
are carefully withdrawn into the peritoneal cavity.
|
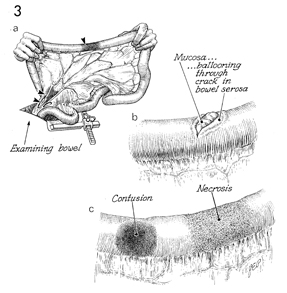
The entire small bowel is carefully
inspected from the ileocecal junction to the ligament of Treitz.
In a are areas
of devascularization and laceration in the mesentery that cause
acute loss of blood to the small bowel. In b,
a potential enterotomy with laceration of the serosa and muscularis
is causing the intestinal mucosa to balloon through a crack in
the bowel serosa. Contusions and necrosis are depicted in c. |
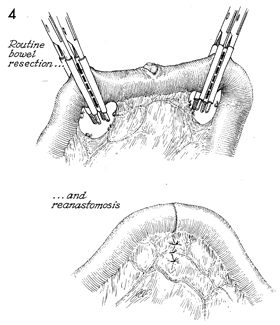
It is wise for the surgeon to resect
all areas of contusion, necrosis, and enterotomy and to carefully
inspect the vasculature in the small bowel mesentery. Linen-shod
clamps are placed in an oblique fashion away from the defect
to ensure that the antimesenteric border of the small bowel used
in the anastomosis will have an excellent blood supply.
The anastomosis is performed according
to the Gambee or stapler technique as indicated in the section
Small Bowel. The insert shows
the mesentery plicated with interrupted absorbable suture. |
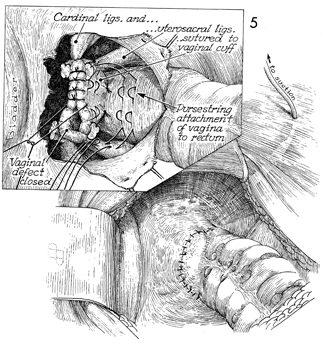
The opening in the vagina through which
the evisceration occurred is shown. After the small bowel has
been adequately inspected and cared for, the defect in the
pelvis must be repaired. The important structures shown here
are the cardinal ligaments, uetrosacral ligaments, anterior
rectum, and vagina. The cardinal ligaments should be reapproximated
to the angles of the vagina. The vaginal defect itself should
be closed with 0 synthetic absorbable suture.
The cul-de-sac should be obliterated
by several 0 synthetic absorbable sutures placed in the posterior
vaginal wall through the uetrosacral ligaments, the anterior
wall of the rectum, the uetrosacral ligament on the opposite
side, and back to the posterior vaginal wall. After all of these
sutures have been placed, they should be progressively tied from
the deepest to the most superficial.
The pelvic peritoneum should
be reconstructed. If there has been any contamination from intestinal
contents, a suction drain should be placed in the pelvis.
|
|
|
