
Malignant
Disease:
Special Procedures
Staging
of Gynecologic
Oncology Patients With
Exploratory Laparotomy
Subclavian Port-A-Cath
Peritoneal Port-A-Cath
Application
of Vaginal
Cylinders for Intracavitary
Radiation Therapy
Application
of Uterine Afterloading Applicators
for Intracavitary Radiation Therapy
Pelvic High-Dose
Afterloader
Abdominal
Injection of Chromic Phosphate
( ) )
Supracolic
Total Omentectomy
Omental Pedicle "J"
Flap
Tube Gastrostomy
Total Vaginectomy
Radical
Vulvectomy
With Bilateral Inguinal
Lymph Node Dissection
Reconstruction
of the
Vulva With Gracilis Myocutaneous Flaps
Transverse
Rectus
Abdominis Myocutaneous
Flap and Vertical Rectus
Abdominis Myocutaneous
Flap
Radical
Wertheim
Hysterectomy With
Bilateral Pelvic Lymph
Node Dissection and With Extension of the Vagina
Anterior Exenteration
Posterior Exenteration
Total Pelvic
Exenteration
Colonic
"J" Pouch Rectal
Reservoir
Kock Pouch
Continent Urostomy
Omental "J" Flap
Neovagina
Ileocolic
Continent Urostomy (Miami Pouch)
Construction
of Neoanus
Gracilis Dynamic Anal
Myoplasty
Skin-Stretching
System Versus Skin Grafting
Gastric
Pelvic Flap for
Augmentation of Continent Urostomy or Neovagina
Control
of Hemorrhage in Gynecologic Surgery
Repair
of the Punctured
Vena Cava
Ligation
of a Lacerated
Internal Iliac Vein and
Suturing of a Lacerated Common Iliac Artery
Hemorrhage
Control in
Sacrospinous Ligament
Suspension of the Vagina
Presacral
Space
Hemorrhage Control
What
Not to Do in Case of Pelvic Hemorrhage
Packing
for Hemorrhage
Control
Control
of Hemorrhage
Associated With Abdominal Pregnancy |
Ligation of a Lacerated Internal
Iliac Vein
and Suturing of a
Lacerated Common Iliac Artery
Laceration of a common iliac vein or artery can occur during insertion
of the trocar and sleeve with laparoscopy or can occur with lymph node
dissection for cancer.
Technique
METHODS COMMON TO BOTH LIGATION AND SUTURING
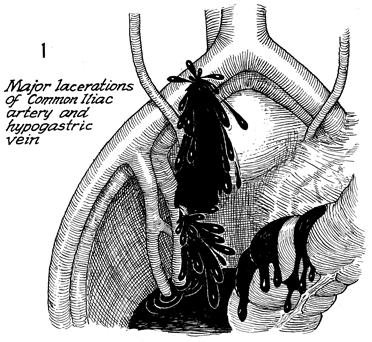
The most common site for laceration of the
common iliac artery is generally on the right side, as shown
here, because most surgeons are right-handed and insert the laparoscopic
trocar with the right hand. At the bottom, the internal iliac
(hypogastric) vein is shown lacerated, with copious bleeding
coming from both sites. |
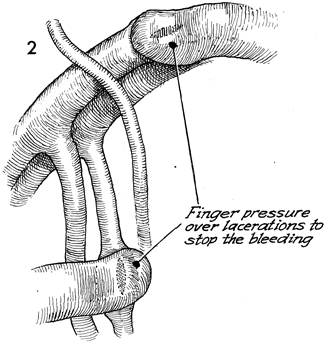
The first step any surgeon should utilize
is placing the finger over the laceration of the artery or vein.
Note the proximity of the right ureter to both the right common
iliac artery and the right common iliac vein. |
LIGATION OF A LACERATED INTERNAL ILIAC VEIN
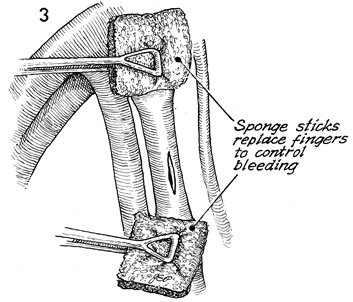
Every laparotomy kit contains
sponge sticks. Sponge sticks can be used for proximal and distal
pressure against the lacerated vessel, whether it be the internal
iliac vein, as shown here, or the common iliac artery, as shown
in Figure 2.
Blood flow through the open
vessels must be controlled. Do not attempt to suture a large
blood vessel while copious volumes of blood are flowing. |
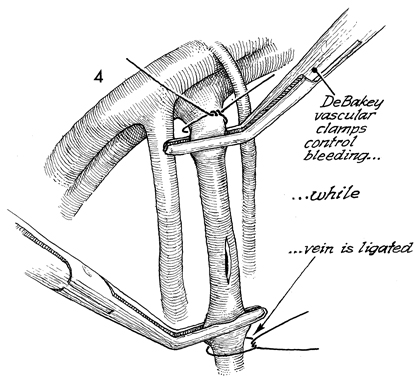
Ligation of a lacerated vein
can be more difficult than suturing of a lacerated artery.
The internal iliac vein can be tied off without sequela. Here,
DeBakey vascular clamps are placed proximal and distal on the
vein laceration. The vein is tied off at the proximal and distal
ends with synthetic absorbable suture. Collateral venous drainage
will develop between the lower extremity and the ligated internal
iliac vein. |
SUTURING OF A LACERATED COMMON ILIAC ARTERY
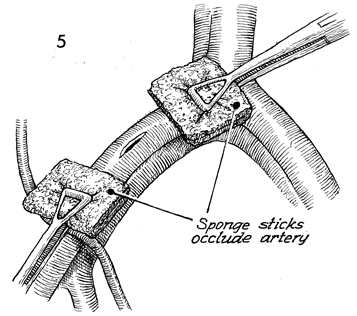
Sponge sticks can also be
used to control hemorrhage from a lacerated right common iliac
artery. The artery must be repaired with suture. Blood flow
must be controlled. Suturing an open artery is inaccurate and
poor technique.
Sponge sticks are always available
in laparotomy kits. Often, proper vascular instruments are
not. It is a serious mistake to use Kelly, Ochsner, or Kocher
clamps on large arteries or veins that need to be sutured. |
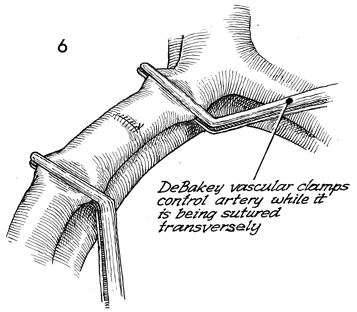
Figure 6 illustrates the proper
way to repair a common iliac artery. DeBakey vascular clamps
are placed proximal and distal to the site. When the bleeding
ceases, a proper closure is made in the transverse plane of
the vessel with 5-0 synthetic monofilament permanent suture
on a cardiovascular needle. The 5-0 Prolene with a cardiovascular
needle frequently comes in double-tipped needle at both ends
of the suture. This allows a running suture that everts rather
than inverts the suture line in the artery. Inversion may produce
eddy currents that may cause blood clots. |
|
